

Hello,
Dr. Batman
Hello Doctor, Welcome!
Profile
Name: Batman
Email: batman@gotham.com
ANATOMY
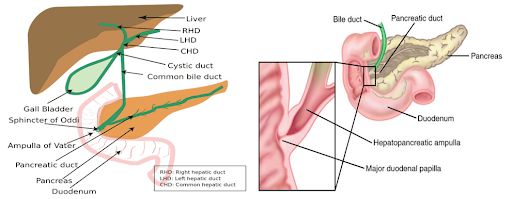
(Total Questions - 82)Q.1. A 31 year old female with known gallstones undergoes a cholecystectomy. Unfortunately, she continues to have pain, and her liver function tests suggest an obstructive jaundice. An ERCP is performed which demonstrates a calculus lodged in the second part of the duodenum. What is the most likely place that the stone was lodged?
Correct Answer : B
This question is purely testing your knowledge of the biliary tree anatomy. The Hepatopancreatic ampulla, otherwise known as the Ampulla of Vater, is formed from the pancreatic duct and the common bile duct. It opens into the second part of the duodenum.
Q.2. Which of the following is located at the level of the first lumbar vertebra (L1)?
Correct Answer : A
The first lumbar vertebrae is level with the anterior end of the ninth rib. This level is also called the important transpyloric plane since the pylorus is at this level. Other important structures are also located at this level, they include; the fundus of the gall bladder, coeliac trunk, superior mesenteric artery, termination of spinal cord, and hilla of kidneys.
The Transpyloric plane, also known as Addison’s Plane, is an upper transverse line, located halfway between the jugular notch and the upper border of the pubic symphysis.
The plane in most cases cuts through the pylorus of the stomach, the tips of the ninth costal cartilage, and the lower border of the first lumbar vertebra.
Q.3. What anatomical structure or landmark lies just above the midpoint of the inguinal ligament?
Correct Answer : C
The deep inguinal ring is located about 2.5 cm above the midpoint of the inguinal ligament.
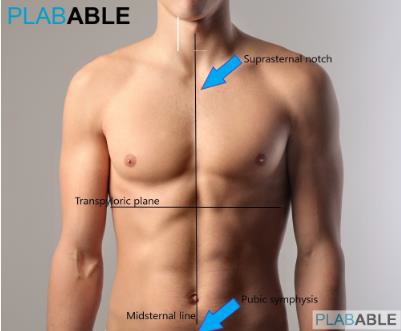
Q.4. Which landmark or anatomical structure is located at the midpoint between the suprasternal notch and pubic symphysis?
Correct Answer : D
The suprasternal notch (fossa jugular sternalis) is also known as the jugular notch. The Transpyloric plane, also known as Addison’s Plane, is an upper transverse line, located halfway between the jugular notch and the upper border of the pubic symphysis. The plane in most cases cuts through the pylorus of the stomach,
the tips of the ninth costal cartilages, and the lower border of the first lumbar vertebra While it is true that the transpyloric plane passes through the fundus of the gallbladder,
the fundus of the gallbladder is NOT at the midpoint between the suprasternal notch and pubic symphysis. It is on the same plane but it is more lateral nearer to the midclavicular line rather than the midsternal line.
Q.5. A 24 year old patient was lying down on the operating table in a position with his arms hanging down for 3 hours. Soon after he woke up, he complains of numbness and weakness on his left hand and has a wrist drop. There is a loss of sensation over a small area between the dorsal aspect of 1st and 2nd metacarpals. What is the most likely structure to be damaged?

Correct Answer : C
Radial nerve(C5-T1)Motor to• Extensor muscles (forearm, wrist, fingers, thumb)• If damage leads to wrist dropSensory to• If damaged – Sensory loss is variable but always includes the dorsal aspect of the root of the thumb. Usually leads to loss to a small area between the dorsal aspect of 1st and 2nd metacarpals.
It is important to remember the key phrases for nerve damage during exam. There are certain phrases you need to memorize to relate them to specific nerve damage.ExamplesWrist drop – Radial nerveFoot drop – Either common peroneal nerve or sciatic nerveClaw hand – Ulnar nerveParaesthesia of thumb, index, and middle finger
– Median nerveNumbness on the superior aspect of the upper arm just below the shoulder joint – Axillary nerveFibular neck fracture – Common peroneal nerveFemur neck fracture or Acetabular fractures
– Sciatic nerveFracture of the humeral shaft – Likely Radial nerveFracture of the humeral neck
– Likely Axillary nerveMonteggia fracture – Radial nerve. Paraesthesia and impaired sensation in both hands (glove distribution) – Peripheral neuropathy.
Q.6. A 35 year old man sat cross-legged for 30 minutes after which he found himself unable to dorsiflex his left foot and had loss of sensation in the web space between the big toe and the second toe. What is the most likely anatomical structure to be affected?
Correct Answer : D
Deep peroneal nerve (Deep fibular nerve) Motor functions The deep peroneal nerve innervates the muscles in the anterior compartment of the leg which are responsible for dorsiflexion of the foot at the ankle joint. Sensory functions The deep peroneal nerve innervates the webbed space of skin between the great toe (hallux) and the second toe.
Clinical relevance- The deep peroneal nerve can become entrapped or compressed during its course through the anterior compartment of the leg, and so a patient loses the ability to dorsiflex the foot. With unopposed plantarflexion, their foot drops. There are two main reasons why the deep fibular nerve could be compressed
. • The first is that the anterior leg muscles have been excessively used and so are compressing the nerve with the anterior compartment. The patient will experience pain in the anterior leg.
• The other common cause is tight-fitting shoes, compressing the nerve beneath the extensor retinaculum. This commonly occurs with wearing tight ski boots (referred to as ski boot syndrome).
The patient will experience pain in the dorsum of the foot.
Q.7. A 55 year old man with a history of a stroke a year ago has severe difficulty remembering events in his life. This includes important events like the year he married his wife. Along with the long term memory impairment, he has altered sexual behaviour which has been seen after the stroke. He is also noted to have a visual defect after the stroke. What is the most likely visual defect?
Correct Answer : C
This man has had a stroke affecting his temporal lobe. It is important to note that the most common cause of temporal lobe lesions is a cerebrovascular event (CVE). Several neural structures found in the temporal lobe are proposed to be involved in memory.
This also includes structures closely related to it such as the amygdala, the hippocampus, and the rhinal cortex in the temporal lobe. Once you know that the temporal lobe is affected, you will be able to answer the question.
The optic radiation passes through the temporal lobes. Damage to this can cause an upper homonymous quadrantanopias.
Q.8. A 37 year old man has a nonhealing ulcer on the skin of the right medial malleolus. Which lymph node is likely to be involved?
Correct Answer : A
The skin at the medial malleolus drains into inguinal lymph nodes.
Q.9. A 60 year old man was screwing his cupboard to the wall when he suddenly felt a rupture at the cubital fossa resulting in a swollen elbow with weakness on flexion and supination. A lump in the distal arm is seen. What is the most likely diagnosis?
Correct Answer : C
The weakness and lump at the distal arm are characteristic of a biceps tendon rupture. There are two types of biceps tendon rupture which are proximal and distal.
Thankfully, this question does not require you to differentiate the two.
Proximal biceps tendon rupture
• Ruptures of the proximal biceps tendon make up nearly all biceps ruptures
• Presents with the biceps muscle bunches up in the distal arm, causing the characteristic ‘Popeye muscle’ appearance.
There is minimal loss of function. Distal biceps tendon rupture
• Distal biceps tendon rupture is usually caused by a single traumatic event involving flexion against resistance, with the elbow at a right angle.
• Presents with a sudden tearing sensation resulting in a painful swollen elbow with weakness of flexion and supination.
Q.10. What important landmark is found above the 5th intercostal space and anterior to the mid axillary line?
Correct Answer : B
This landmark is especially important when attempting to insert a chest drain. Always look for the safe triangle when inserting chest drains. Insert the drain in an area anterior to the mid-axillary line, posterior to the pectoral groove, and above the 5th intercostal space.
Q.11. A camel rider sustained an injury to the lateral side of his right leg just below the knee caused by the camel stick. The site is slightly bruised and tender to touch. He is unable to either dorsiflex or evert the foot. There is loss of sensation over the front and outer half of the leg and dorsum of the foot. What is the most likely anatomical structure to be affected?
Correct Answer : A
This is called a peroneal strike. A peroneal strike is a temporarily disabling blow to the common peroneal nerve of the leg,
just above the knee which causes a temporary loss of motor control of the leg, accompanied by numbness and a painful tingling sensation from the point of impact down the leg, usually lasting anywhere from 30 seconds to 5 minutes in duration.
Q.12. A 32 year man presents to A&E with a fracture dislocation of his right elbow. He complains of loss of sensation in his little finger and ring finger. Which is the most likely nerve to be involved?
Correct Answer : B
Ulnar nerve (C8-T1) Sensory loss is over the little finger and a variable area of the ring finger (palmar & dorsal) This is the nerve of finger abduction and adduction. Injury level determines the severity of the claw deformity. In a distal lesion of the ulnar nerve,
there will be more clawing of the 4th and 5th fingers compared with a proximal, more complete lesion at the elbow.
Q.13. A 75 year old woman was referred by her general practitioner to the same day ophthalmology clinic because of a 4 hour history of sudden painless loss of vision affecting her right eye. Her medical history includes hypertension and heavy smoking. Ophthalmic assessment showed visual acuity of light perception only in the right eye and 6/9 in the left eye. Apart from early questioning, the patient admitted that she had previously experienced episodes of vision loss in the same eye, which lasted for a few seconds to a few minutes. What is the most likely artery involved in this scenario?
Correct Answer : D
Patients with central retinal artery occlusion have a sudden painless loss of vision, usually within the initial visual acuity of counting fingers or worse. Urgent management is required. The short episodes of previous vision loss are termed amaurosis fugax.
This temporary painless type of vision loss produces loss of vision in up to 10% of patients with central artery occlusion.
Amaurosis fugax is usually caused by emboli coming from atherosclerotic carotid artery resulting in a fleeting loss of vision when the emboli pass through the retinal circulation. Any temporary reduction in the retinal artery blood flow would cause retinal hypoxia which includes any emboli arising from vasculature preceding the retinal artery. The anatomy of the arterial supply of the eye is complicated. It is provided by several branches of the ophthalmic artery, which derives from the internal carotid artery. These branches include the central retinal artery, the short and long posterior ciliary arteries, and the anterior ciliary arteries. The retina is mainly supplied by the central retinal artery and its branches which is a site of emboli.
The other arteries are less likely to be involved as they present with additional symptoms.
• Anterior and middle cerebral artery occlusions have features of contralateral hemiparesis and sensory loss.
• Posterior inferior cerebellar artery has features of ipsilateral facial pain and temperature loss, contralateral limb/torso pain and temperature loss, ataxia, and nystagmus
• Anterior communicating artery is a common site for brain aneurysms and if large enough to compress the optic chiasm visual defects such as bitemporal hemianopsia may occur Key points to remember
• Amaurosis fugax is the temporary loss of vision due most commonly to ischaemia
• Embolism is the most common cause of central retinal artery occlusion with the major source of this being atherosclerotic plaques of the carotid artery (as opposed to transient ischaemic attacks (TIA) involving the cerebral hemispheres where emboli usually originate from heart disease instead of carotid stenosis).
Q.14. A 45 year old man has been informed by his doctors that he has a carcinoma of the head of the pancreas. Which structure is in close proximity with the head of pancreas?
Correct Answer : C
The Common Bile Duct lies in close relation to the head of the pancreas. The initial presentation on about 70% of patients with carcinoma of the head of the pancreas is jaundice due to obstruction of the CBD by the tumour.
Q.15. A 58 year old man underwent surgery for varicose veins of the leg. He is now complaining of numbness on the medial side of his foot. What is the most likely nerve involved?
Correct Answer : D
The Saphenous nerve is the largest cutaneous branch of the femoral nerve and is a strictly sensory nerve with no motor functions. Surgery for varicose veins, saphenous vein cutdown, and orthopedic surgery can result in damage to the saphenous nerve, resulting in loss of cutaneous sensation in the medial leg.
It can also be damaged during vein harvest for bypass surgery and trocar placement during knee arthroscopy. Remember:
• Loss of sensation in the medial foot: Saphenous Nerve
• Loss of sensation in the lateral foot: Sural nerve
• Foot drop: Common peroneal nerve.
Q.16. A 33 year old man suffered a mandibular fracture and now has loss of sensation over the chin and mucosal surface of the lower lip. Which nerve is most likely to be involved?
Correct Answer : B
The Inferior Alveolar Nerve is a branch of the Mandibular nerve, which is the third branch of the Trigeminal Nerve. The nerve supplies sensation to the lower teeth and via the mental nerve, sensation to the chin and lower lip. Damage can occur commonly during dental procedures especially wisdom teeth removal as well as due to mandibular trauma.
Q.17. A 24 year old man is hit by a baton just above the knee on his right leg. This is followed by loss of motor control of the leg. His foot drops and is unable to dorsiflex his foot. There is loss of sensation over the front and outer half of the leg and dorsum of the foot. What is the most anatomical structure to be affected?
Correct Answer : A
This is called a peroneal strike. A peroneal strike is a temporarily disabling blow to the common peroneal nerve of the leg, just above the knee which causes a temporary loss of motor control of the leg, accompanied by numbness and a painful tingling sensation from the point of impact down the leg, usually lasting anywhere from 30 seconds to 5 minutes in duration.
Q.18. A 32 year old woman has weakness of both her hands and neck pain immediately after a fall down a flight of stairs. She was brought in by a scoop stretcher by the paramedics with a hard cervical collar, adhesive tape and sandbags to immobilize the neck. An X-ray was ordered. Which is the lowest vertebrae that needs to be seen in a lateral cervical X-ray to help diagnose the injury?
Correct Answer : C
Hand weakness involves either the median nerve which has contributions from C5-T1 or the ulnar nerve which originates from the C8-T1 nerve roots. Remember, a C8 vertebrae does not exist so the option for C8/T1 is wrong. There are seven cervical vertebrae (C1-C7) and a total of eight cervical nerves C1-C8.
All cervical nerves except C8 emerge above their corresponding vertebrae, while the C8 nerve emerges below the C7 vertebra which is between C7 and T1 vertebrae. When you request a cervical X-ray for any severe injury of the neck, you would like the film to extend up to C7/T1 as you would be able to see the cervical vertebrae (C1-C7). This applies to any trauma including road traffic accidents.
The patient should not try to move her neck and she should continue to have the cervical collar and immobilization of the neck until the cervical X-ray is performed to rule out cervical fractures.
In this case, there should be at least 3 X-ray views taken.
• AP cervical spine view which shows the pedicles, facets, and lateral masses
• Lateral cervical spine view
• Open-mouth odontoid view also called the peg view would demonstrate peg fractures In some cases where the patient’s neck is short, the X-ray film would not show the C7/T1 junction.
The radiographers would then ask for a swimmer's lateral view.
This involves repositioning the patient in such a way that the arm closest to the sensor is placed above the patient’s head much like a swimming position. This would likely provide a clear visualization of the C7/T1 junction.
If again, this does not capture that junction, then we would need to request a CT scan to rule out fractures.
Q.19. A 62 year old male comes to the GP complaining of double vision when climbing down the stairs. Which is the most likely nerve to be affected?
Correct Answer : D
The trochlear nerve innervates the superior oblique muscle. It only causes diplopia on downgaze like looking downwards to walk. This is a high-yield question in exam. Please remember the nerves involving the eye and how they present.
NERVES INVOLVING THE EYE Functions CN III – Oculomotor nerve
• Controls most of the eye muscle
• Constriction of pupil
• Levator palpebrae superioris CN IV – Trochlear nerve
• Innervates a single muscle – Superior oblique CN VI – Abducens nerve
• Lateral rectus muscle Palsies The simple method to remember for the exam is: CN III – Oculomotor nerve
• Will have features of either ptosis and/or a dilated pupil on the nerve on the same side as the affected eye
• Mnemonic: The letter “O” for oculomotor which with a good imagination can represent a dilated pupil CN IV – Trochlear nerve
• Diplopia on downward gaze
• If looks right and sees double, then the lesion is on the left (Opposite to gaze) CN VI – Abducens nerve
• If the looks left and see double, then the lesion is on the left. (same side as gaze) Another mnemonic is: LR6(SO4)O3
• Lateral rectus – 6th Nerve
• Superior oblique – 4th Nerve
• Others – 3rd Nerve.
Q.20. A 33 year old man complains of double vision when he looks to the right. Which is the most likely nerve to be involved?
Correct Answer : B
His right eye is unable to abduct thus he sees double. The nerve involved here would be the right abducens nerve.
Q.21. A 32 year old patient presents to Accident & Emergency with a deep cut on the surface of her palm and the surface of the back of her wrist. She has an inability to extend the distal phalanx of her ring finger. What is the most likely structure affected?
Correct Answer : A
Unfortunately, this is just something that you have to memorize Some other important clinchers for anatomy questions:
Ulnar nerve (C8-T1) Sensory loss is over the little finger and a variable area of the ring finger (palmar & dorsal) This is the nerve of finger abduction and adduction. Injury level determines severity of the claw deformity.
In a distal lesion of the ulnar nerve, there will be more clawing of the 4th and 5th fingers compared with a proximal, more complete lesion at the elbow. The short saphenous vein is the only one which travels on the lateral aspect of the ankle. Note that the great or long saphenous vein travels on the medial aspect of the ankle.
The left anterior descending (LAD, interventricular artery appears to be a direct continuation of the left coronary artery which descends into the anterior interventricular groove. The skin at the medial malleolus drains into inguinal lymph nodes. The first lumbar vertebra is level with the anterior end of the ninth rib. This level is also called the important transpyloric plane, since the pylorus of the stomach is at this level. The deep inguinal ring is located about 2.5 cm above the midpoint of the inguinal ligament. Full extension of right thumb is achieved by extensor pollicis longus The fundus of the gall-bladder approaches the surface behind the anterior end of the ninth right costal cartilage close to the lateral margin of the Rectus abdominis. The extensor digitorum communis extends the phalages, then the wrist, and finally the elbow. It tends to separate the fingers as it extends them. The suprasternal notch (fossa jugularis sternalis) is also known as the jugular notch The extensor pollicis brevis extends the thumb at the metacarpophalangeal joint. Whenever you see the word “foot drop” or “unable to dorsiflex: pick the peroneal nerve. Radial nerve (C5-T1) Motor to • Extensor muscles (forearm, wrist, fingers, thumb) • If damaged –
leads to wrist drop Sensory to
• If damaged – Sensory loss is variable, but always includes the dorsal aspect of the root of the thumb.
Usually leads to loss to a small area between the dorsal aspect of 1st and 2nd metacarpals. Facial nerve lesion leads to facial weakness and loss of taste sensation in the anterior two-thirds of the tongue. Vagus nerve lesion results in weak cough, vocal cord paralysis with dysphonia. There is also parasympathetic loss of innervation to respiratory, gastrointestinal, and cardiovascular systems.
Trigeminal nerve lesion presents with signs depending upon the level of the lesion. Usually, there is weakness of muscles of mastication, jaw deviates to the side of weak pterygoid muscle and there is also loss of sensation on the face.
Glossopharyngeal nerve lesion presents with loss of gag reflex, loss of taste sensation from the posterior third of the tongue, and loss of general sensation from the posterior pharynx, tonsils, and soft palate. The hypoglossal nerve is the twelfth cranial nerve XII and innervates muscles of the tongue.
Q.22. Which artery descends into the anterior interventricular groove?
Correct Answer : D
The left anterior descending (LAD, interventricular) artery appears to be a direct continuation of the left coronary artery which descends into the anterior interventricular groove.
Q.23. A 45 year old man presents to the clinic with herpes zoster over the dermatome of the maxillary branch of the trigeminal nerve. Which type of mucosa will be affected along with the dermatome?
Correct Answer : A
To choose the correct answer, one should remember the maxillary nerve and the structures that it supplies. The maxillary nerve carries sensory information from the lower eyelid and cheek, the nares and upper lip, the upper teeth and gums, the nasal mucosa,
the palate and roof of the pharynx, the maxillary, ethmoid and sphenoid sinuses, and parts of the meninges. The maxillary division of the facial nerve innervates both the cheek and the palate (along with the upper lip, upper teeth, gums, nasal mucosa, roof of the pharynx, and the maxillary ethmoid and sphenoid sinuses).
But pay attention, the question asks about which MUCOSA the maxillary branch of the trigeminal nerve innervates so the best answer will therefore be the palate as it is a mucous membrane.
Q.24. A 73 year old woman with rheumatoid arthritis is unable to extend the fingers of her right hand at the metacarpophalangeal joint and interphalangeal joints following a fall. What is the most likely tendon to have been damaged?
Correct Answer : C
The extensor digitorum communis extends the phalanges, then the wrist, and finally the elbow. It tends to separate the fingers as it extends them.
Q.25. A 46 year old man is being treated for a pleural effusion. A chest drain has been sited just below the 4th rib, anterior to the mid-axillary line on his right side. What structure is at particular risk of injury?
Correct Answer : A
When inserting a chest drain, one needs to be aware of the intercostal neurovascular bundle. This is located at the inferior aspects of the ribs. The intercostal neurovascular bundle contains structures in a specific order which can be remembered as “VAN”.
This stands for • V – Vein • A – Artery • N – Nerve This order is from top to bottom The options in this question only have one of the structures of the intercostal neurovascular bundle which is the intercostal artery.
Hence that is the answer. Having this knowledge of the location of the intercostal neurovascular bundle would help you remember to insert the needle directly above the upper margin of the relevant rib.
Chest drain Insertion technique Chest insertion should be performed within the “safe triangle” In the exam, it is important to remember the borders of the “Safe triangle” which is used in clinical practice for chest drain insertions.
It is bounded anteriorly by the pectoralis major, posteriorly by latissimus dorsi, inferiorly by the fifth intercostal space, and superiorly by the axilla. By inserting at the safe triangle, we avoid major vessels and muscles
. It is important to note that the intercostal vessels and nerves run below the inferior border of the ribs. Thus, the drain track should be directed over the top of the lower rib to avoid the intercostal vessels lying below each rib.
Q.26. A 53 year old man has reduced sensation on the medial and posterior aspect of his lower left forearm and tingling described as “pins and needles” in his left hand. He also has weakness of thumb extension and wrist ulnar deviation. There is wasting of the muscles of the left hand. What is the most likely structure affected?
Correct Answer : D
The C8 nerve root exits the spinal cord at the C7-T1 spinal segment. If the C8 nerve becomes compressed or irritated for any reason, then C8 radiculopathy will occur. Symptoms of a C8 radiculopathy include weakness of thumb extension and wrist ulnar deviation. Paresthesias in the little finger is also a finding in C8 radiculopathy. The test to be performed to identify C8 radiculopathy is to have the patient hold their extended fingers together against the examiner’s attempts to open the fingers.
It is important in this question to differentiate between pure ulnar neuropathy and C8-T1 radiculopathies.
The ulnar nerve provides sensation to the fourth and fifth fingers and medial border of the hand. The ulnar nerve innervates all intrinsic hand muscles, except the abductor and flexor pollicis brevis, opponens pllicis, and lateral two lumbricals, which are innervated by C8 and T1 via the median nerve.
By examining these five muscles, one can clinically differentiate cubital tunnel syndrome from C8-T1 radiculopathies. The ulnar nerve does not provide sensation to the medial forearm,
which is innervated by the medial antebrachial cutaneous nerve which is supplied by C8 and T1 via the medial cord of the brachial plexus.
Therefore, an ulnar lesion at the elbow which is a common site of compression or trauma would result in anaesthesia of the ulnar hand and fingers but not the forearm.
Q.27. A 64 year old woman has difficulty in moving her right shoulder on recovering from surgery of the posterior triangle of her neck. What is the most likely anatomical structure to be affected?
Correct Answer : B
The accessory nerve is a cranial nerve that controls the sternocleidomastoid and trapezius muscles. Injury to the spinal accessory nerve can cause an accessory nerve disorder or spinal accessory nerve palsy, which results in diminished or absent function of the sternocleidomastoid muscle and upper portion of the trapezius muscle.
Q.28. A 55 year old man presents with an ulcer of the scrotum. Which is the most likely lymph node involved in it’s lymphatic drainage?
Correct Answer : A
The superficial inguinal lymph nodes receive afferent lymphatic vessels from the scrotum.
Q.29. A 72 year old woman has had a stroke a month ago. Since then she has had left upper and left lower limbs which are paralyzed and she has difficulty in speaking. Which is the most likely anatomical site to be affected?
Correct Answer : C
For the exam, know these three general areas of infarct. Cerebral infarct
• Contralateral sensory loss/hemiplegia, dysphasia, homonymous hemianopia.
Brainstem infarct
• Quadriplegia, locked-in syndrome, vertigo, diplopia Lacunar infarcts
• Ataxic hemiparesis, pure motor loss, pure sensory loss, sensorimotor loss, dysarthria Although this patient is having difficulty speaking, the most likely area of fact is still the internal capsule (which is part of the lacunes).
Q.30. A 35 year old man is due for a surgery to attempt to removal of a glioma. What is the most likely anatomical structure to be opened durign the surgery?
Correct Answer : A
Gliomas are tumours arising from glial cells and may occur in the spinal cord or the brain.
The dura mater, which is a thick membrane of the outermost three layers of the meninges that surround the brain and
spinal cord would need to be opened for the surgery to take place.
Q.31. A 69 year old woman has been diagnosed with left ovary carcinoma. What lymph nodes are likely to be removed?
Correct Answer : C
The lymphatic drainage of the ovaries is into the para-aortic nodes.
Q.32. A 68 year old woman is unable to extend the interphalangeal joint of her right thumb six weeks following a fracture of the right radius. The other fingers and thumb movements are unaffected. What is the most likely tendon to be damaged?
Correct Answer : C
Full extension of the right thumb is achieved by extensor pollicis longus.
Q.33. A 12 year old boy presents with a painful swollen knee after a sudden fall on his right knee. The pain is localized below the knee cap. Which anatomical structure is most likely to be affected?
Correct Answer : B
Prepatellar bursa The prepatellar bursa is a frontal bursa of the knee joint. It is a superficial bursa with a thin synovial lining located between the skin and the patella. Prepatellar bursitis classically occurred in housemaids, hence the nickname ‘housemaid’s knee’.
It is commonly seen in people who have knees such as plumbers. Friction caused by repeated kneeling can cause it.
It is a common cause of swelling and pain over the anterior inferior patella.
Symptoms
• Redness
• Inability to flex the knee
• Pain and swelling are localized over the site of the bursa (e.g. below the patella) Rest usually relieves symptoms.
Q.34. A 34 year old man has a white patch on the margin of the mid-third of his tongue. Which is the most likely lymph node involved?
Correct Answer : C
The anterior 2/3 of the tongue is supplied by the submandibular lymph nodes. The posterior 1/3 of the tongue is supplied by the jugulo-omohyoid lymph nodes The tip of the tongue is supplied by the submental lymphnodes.
Q.35. A 45 year old man has a cancer of the posterior oropharynx. What is the most likely lymph node to be involved?
Correct Answer : B
The posterior oropharynx predominantly drains into the jugular nodes. The jugular nodes are also known as the deep cervical nodes though that is an outdated terminology.
Q.36. A 36 year old male involved in a street fight presents to Accidents and Emergency with bruises and deformity of his lower right knee. He was given pain relief and an X-ray was ordered. The X-ray shows a fracture of the neckof the fibula. What is the most associated nerve injury?
Correct Answer : C
Peroneal nerve injury • The common peroneal nerve crosses the fibular neck and is susceptible to injury from a fibular neck fracture, the pressure of a splint, or during surgical repair. • Peroneal nerve injury may result in foot drop and sensation abnormalities.
Q.37. You are observing a medical student perform a neurological examination on a patient. They forget to perform the reflexes so you decide to quiz them on their neuroanatomy. Which of the following reflexes and innervating spinal nerves are correctly paired?
Correct Answer : D
It is important to understand the nerve root innervation of the common reflexes. This is not always an exact science, and there may be slight variations depending on which textbook you read. Damage to the associated nerves can also lead to diminished reflexes.
REFLEX ACTION INNERVATION Anal (anal wink) reflex Contraction of external anal sphincter muscle on stroking the skin around the anus S2-S4 Ankle reflex The Achilles tendon is struck causing plantar flexion of the foot S1&S2 Sciatic nerve Knee (patella) reflex The patellar ligament is struck causing contraction of the quadriceps muscle L3 & L4 Femoral nerve Biceps reflex
The biceps brachii tendon is struck causing flexion at the elbow C5 & C6 Musculocutaneous nerve Brachioradialis (supinator reflex)
The brachioradialis is struck causing wrist extension with radial deviation C6 & C7 Radial nerve Triceps reflex The triceps brachii tendon is struck causing extension C6 & C7 Radial nerve.
Q.38. A 23 year old man is having difficulty in speaking following a stab wound to the right of his neck. On tongue protrustion test, the tip of tongue is deviated to the right. Which of the following nerve is the most likely to be affected in this patient?
Correct Answer : C
The hypoglossal nerve is the twelfth cranial nerve XII and innervates muscles of the tongue. The following are the common causes of this nerve injury: a. Lower motor neuron lesions – Polio, syringomyelia b. Stroke c. Bulbar Palsy d. Neck trauma e.
Surgery – Carotid endarterectomy Symptoms often show deviation of the tongue towards the paralyzed side when it is stuck out. This is because of the weaker genioglossal muscle. Other lesions: Facial nerve lesion leads to facial weakness and loss of taste sensation in the anterior two third of the tongue. Vagus nerve lesion results in weak cough, vocal cord paralysis with dysphonia.
There is also parasympathetic loss of innervation to respiratory, gastrointestinal, and cardiovascular systems.
Trigeminal nerve lesion presents with loss of gag reflex, loss of taste sensation from the posterior third of the tongue, and loss of general sensation from the posterior pharynx, tonsils, and soft palate.
Q.39. What anatomical landmark correlates to the tip of the 9th costal cartilage?
Correct Answer : C
The fundus of the gallbladder approaches the surface behind the anterior end of the ninth right costal cartilage close to the lateral margin of the Rectus abdominis.
Q.40. A 63 year old woman presents to the Emergency Department with an inability to flex the proximal interphalangeal joint of her fingers of the left hand. Upon further questioning, she reveals that she has broken a wine glass and caused a cut on the surface of her left hand. She also had no previous procedure done to her hand. On examination, there was 2x2 cm clean cut on the left hand. Extension at wrist joint was normal with no problem in adduction and abduction of the hand. However, she was unable to flex her first metacarpophalangeal joint. An X-ray of the left hand was done which was normal. What structure is most likely to be injured in her case?
Correct Answer : A
The correct answer is Flexor digitorum superficialis because it causes flexion at metacarpophalangeal joints (MCP), as well as at the interphalangeal joint (IP) There is no doubt that flexor pollicis brevis flexes the MCP joint of thumb but here we do not have that as an option. Moreover, the patient is also unable to flex the proximal interphalangeal joints of her left hand.
Hence, flexor digitorum superficialis flexes both, the MCP JOINT as well as the IP JOINTS of the hand so the best answer here is flexor digitorum superficialis. Flexor digitorum profundus causes flexion of the distal interphalangeal joint (DIP), therefore, this is not correct.
Lumbrical muscles are intrinsic muscles of the hand that simultaneously flex the metacarpophalangeal joints and extend the interphalangeal joints. The flexor digiti minimi is a hypothenar muscle that causes flexion of the 5th digit (the little finger) at the metacarpophalangeal joint.
The dorsal interosseous muscles arise between the metacarpal bones and are abductors of the fingers.
Q.41. A 63 year old lady with a BMI of 32 has pigmentation on her legs. Dilated veins could be seen on the lateral aspect of her ankles. Which structure would be involved?
Correct Answer : D
The short saphenous vein is the only one which travels on the lateral aspect of the ankle. Note that the great or long saphenous vein travels on the medial aspect of the ankle.
Q.42. A 15 year old boy complains of double vision when climbing down the stairs. This has occurred since he was hit in the face. The images that he sees appear one above the other. He also notices double vision when he looks to the right. What is the most likely nerve to be affected?
Correct Answer : A
The trochlear nerve innervates the superior oblique muscle. It only causes diplopia on downgaze like looking downwards to walk. It is a trochlear nerve lesion on the left side because he sees double when looking on the right side. This is a high-yield question in exam. Please remember the nerves involving the eye and how they present.
Q.43. What is the lymphatic drainage of the testes?
Correct Answer : D
The lymphatic drainage of the testes is into the para-aortic nodes. Both the male and female gonads drain into the para-aortic nodes. Remember, the testes drain into the para-aortic node but the scrotum drains into the superficial inguinal nodes.
Q.44. A 48 year old main with a known posterior gastric ulcer presents with excruciating pain which subsides after analgesia. 8 days later, he becomes unwell and has a temperature of 38.5 C. A collection in the peritoneum is suspected. Where is the most likely location of the collection?
Correct Answer : A
Posterior gastric ulcers arising from the fundus or body of the stomach erode into the lesser sac behind the stomach. The lesser sac is a potential space and is less effective in sealing off the perforation.
This results in the accumulation of gastric contents and pus resulting in the formation of an abscess which will then pass into the peritoneal cavity through the Foramen of Winslow leading to generalized peritonitis. In contrast, posterior perforation of pyloric and duodenal ulcers results in a retroperitoneal abscess.
Q.45. A 45 year old man was hit on his back by a chair during a fight. He presents with back pain and bruising. The back pain is specifically at the midpoint of the spine at the level of the iliac crest. Which vertebrae is likely to be affected?
Correct Answer : B
L4 is at the level of the iliac crest. Most anaesthetist would know this as the supracristal plane
which is the highest point of the iliac crest typically sits at the level of L4 vertebrae which is a landmark for identification of L4/5 where a lumbar puncture can be performed.
Q.46. A 55 year old man with rheumatoid arthritis struck his hand against a door. On examination, he could extend the interphalangeal joint of his right thumb but the metacarpophalangeal joint of the thumb remained flex. What is the most likely tendon to have been damaged?
Correct Answer : B
The extensor pollicis brevis extends the thumb at the metacarpophalangeal joint.
Q.47. A 33 year old man presents with outward gaze and ptosis of his right eye. He also complains of seeing double. Which is the most likely nerve to be affected?
Correct Answer : C
The nerve involved here would be the right oculomotor nerve. This is a high-yield question in exam. Please remember the nerves involving the eye and how they present.
Q.48. What is the most likely anatomical structure to be pierced when inserting a drain in the mid-axillary line?
Correct Answer : A
Please see Q-25 for Chest Drain Insertion Technique
Q.49. A 32 year old man has complaints of pain on the medial side of his left forearm. There was also associated weakness of finger abduction and finger adduction, as well weakness upon adduction of his thumb. Finger flexion was normal. On inspection, atrophy of the muscles of his left hand was noted. What is the most likely associated injury?
Correct Answer : C
A T1 lesion presents with movement disorders that affect the intrinsic muscles of the hand such as adduction or abduction of the digits. Paraesthesia and pain can also occur along the affected nerve. The cervical spine is comprised of seven vertebrae only.
A C8 vertebral injury is physically impossible and hence cannot be the right answer. A C8 nerve root lesion presents with abnormalities of thumb movement primarily, as well as an inability to extend the elbow against resistance.
T1 radiculopathy has similarities in clinical findings to C8 radiculopathy, so be thankful that the option was C8 vertebral injury and not nerve root injury. The ulnar nerve originates from the C8-T1 nerve roots. Ulnar nerve injury leads to the classic ‘claw hand’ deformity.
Since the ulnar nerve provides sensory innervation to the medial side of the hand, the fifth digit, and the medial half of the fourth digit, injury to it will cause loss of sensation or paraesthesia in those areas.
A C6 lesion affects the sensation of the thumb, flexion of the elbow, and rotation of the forearm. It usually occurs in conjunction with C5 injury. One may see this during the delivery of a baby which is known as Erb’s palsy.
Here are some easy points to remember regarding motor function for cervical roots • Flex elbow – C5 • Extend wrist – C6 • Extend elbow – C7 • Flex fingers – C8 • Adduct and abduct fingers – T1 Try to do the above sequence like a strange dance to help you memorize it.
Q.50. A woman comes with an ulcerated lesion 3 cm in the labia majorum. What is the lymphatic drainage of this area?
Correct Answer : B
The key is B. Superficial inguinal lymph nodes
Q.51. A 12-year-old boy presents with painful swollen knee after a sudden fall. Which bursa is most likely to be affected?
Correct Answer : B
Ans. The key is the B. Prepatellar bursa. [A fall onto the knee can damage the prepatellar bursa. This usually causes bleeding into the bursa sac causing swollen painful knees. Prepatellar bursitis that is caused by an injury will usually go away on its own.
The body will absorb the blood in the bursa over several weeks, and the bursa should return to normal. If swelling in the bursa is causing a slow recovery, a needle may be inserted to drain the blood and speed up the process.
There is a slight risk of infection in putting a needle into the bursa].
Q.52. A 34-year-old man with a white patch on the margin of the mid-third of the tongue. Which is the most appropriate lymph nodes involved?
Correct Answer : C
The key is C.Submandibular lymph nodes
Q.53. A 63-year-old lady with a BMI=32 comes to the ED with complaints of pigmentation on her legs. Examination: dilated veins could be seen on the lateral side of her ankle. Which of the following is involved?
Correct Answer : A
Ans. The key is A. Short saphenous vein. [short saphenous vein travels lateral aspect of the ankle while great or long saphenous vein travels medial aspect of ankle].
Q.54. A 40-year-old woman suddenly collapsed and died. At the post-mortem autopsy, it was found that there a bleed from a berry aneurysm from the circle of Willis. In which space did the bleeding occur?
Correct Answer : A
The key is A. Subarcnoid
Q.55. A 37 year-old-man with an ulcer on the medial malleolus. Which of the following lymph nodes are involved?
Correct Answer : D
The key is D. Inguinal lymph node
Q.56. L1 level, what is the most appropriate landmark?
Correct Answer : D
Ans. The given key is the D. Transpyloric plane. [The termination of the spinal cord is between L1 and L2 (variable between people).
L1 landmark- duodenum first part,
superior mesenteric artery,
hila of both kidneys,
upper border of the pancreas,
splenic artery, pylorus, and
fundus of gall bladder].
Q.57. Midpoint between the suprasternal notch and pubic symphysis. What is the most appropriate landmark?
Correct Answer : D
The key is D. Transpyloric plane
Q.58. Tip of the 9th costal cartilage. What is the most appropriate landmark?
Correct Answer : A
The key is A. Fundus of the gallbladder
Q.59. Just above the mid-inguinal point. What is the most appropriate landmark?
Correct Answer : D
The key is D. Deep inguinal ring.
Q.60. 5th ICS (intercostal space) in the anterior axillary line. What is the most appropriate landmark?
Correct Answer : B
The key is B. Chest drain insertion
Q.61. Which artery runs in the anterior inter-ventricular groove?
Correct Answer : B
The key is B. Left anterior descending artery
Q.62. A 62-year-old man with rheumatoid arthritis struck his hand against a door. He subsequently found that although he could extend the interphalangeal joint of his right thumb, the MCP (metacarpophalengeal joint of the thumb remained flex. What is the most likely tendon to have been damaged?
Correct Answer : D
Ans. The key is D. Extensor pollicis brevis. [Action of extensor pollicis brevis is an extension of thumb at the metacarpophalangeal joint. Extensor pollicis longus extends the terminal phalanx of the thumb].
Q.63. A 55-year-old man presents with an ulcer of the scrotum. Which of the following lymph nodes are involved?
Correct Answer : D
The key is D. Inguinal lymph nodes
Q.64. A 73-year-old woman with RA (rheumatoid arthritis) is unable to extend the fingers of her right hand at the MCP joint and IP joints following a fall. What is the most likely tendon to have been damaged?
Correct Answer : C
Ans. The key is C. Extensor digitorum. [The extensor digitorum extends the phalanges, then the wrist, and finally the elbow. It acts principally on the proximal phalanges].
Q.65. In perforation of a post gastric ulcer, where will the fluid accumulate in the peritoneal cavity?
Correct Answer : C
The key is C. Lesser sac
Q.66. A 55-year-old lady with swelling on the abdomen below the umbilicus on the right side. What is the most appropriate lymph node?
Correct Answer : D
The key is D. Inguinal lymph nodes
Q.67. Which anatomical structure to be pierced during surgery midline port during gallstone removal?
Correct Answer : C
The key is C. Linea alba
Q.68. Inserting a drain in the mid-axillary line. What is the most appropriate anatomical structure?
Correct Answer : D
The key is D. Intercostal muscles
Q.69. Removal of a glioma, which most appropriate anatomical structure will be pierced?
Correct Answer : C
The key is C. Duramater
Q.70. A child is not breathing and intubation failed. At what anatomical site should the incision be made?
Correct Answer : B
The key is B. Cricoid cartilage. [Incision for tracheostomy is done which goes down from cricoid cartilage].
Q.71. A middle aged woman has some weakness of hand after an injury. Which vertebra will be the lowest to be included on cervical XR to diagnose the injury?
Correct Answer : A
Ans. The key is A. C7/T1.
Q.72. A 67-year-old lady with an ulcer on the anal margin. Which is the most appropriate lymph nodes involved?
Correct Answer : D
Ans. The key is D. Inguinal lymph nodes. [Anal canal below the pectinate line is drained into superficial inguinal lymph nodes].
Q.73. The artery that runs along the left AV (atrio ventricular) groove. What is the most appropriate option?
Correct Answer : C
The key is C. Circumflex artery
Q.74. An 89-year-old man presents with carcinoma of posterior oropharynx. Which is the most appropriate lymph node involved?
Correct Answer : D
The key is D. Deep cervical lymph node
Q.75. During a laparoscopic procedure, a trochar is inserted halfway between the umbilicus and the ant superior iliac spine. What are the structures most likely to be pierced?
Correct Answer : D
The key is D. Internal oblique and transverse abdominal
Q.76. The artery that runs in the ant inter-ventricular groove. What is the single most appropriate option?
Correct Answer : B
The key is B. Left ant descending artery
Q.77. In a laparoscopic mesh repair for hernia, when the trochar is inserted at midpoint between umbilicus and ischial spine. What structure will be pierced?
Correct Answer : D
The key is D. External and internal oblique muscles
Q.78. A patient has loss of sensation on the tip of her tongue and the inner aspect of the lip. Which nerve is most likely to be involved?
Correct Answer : C
The key is C. Lingual nerve
Q.79. A 40-year-old man presents with headache, vomiting and fever. He has been diagnosed with meningitis. Which of the following is a correct landmark to perform a lumbar puncture?
Correct Answer : B
Ans. The key is the B. Iliac crest. [Lumbar puncture is done in the L3-L4 interspace by palpating the right and left posterior superior spines of the iliac crest and moving the fingers medially towards the spine].
Q.80. A man was involved in a fight and sustained a blow to his mastoid bone. Which one is fractured?
Correct Answer : C
Ans. The key is C. Temporal bone. [The temporal bone consists of four parts— the squamous, mastoid, petrous, and tympanic parts].
Q.81. A 41-year-old woman has varicose vein on the lateral side of her right lower leg. The vein is tortuous and dilated. Which vein is likely to be involved?
Correct Answer : D
D. Short sephanous vein. [Short saphenous vein courses through the lateral side of the leg while long or great saphenous vein courses medially].
Q.82. A 60-year-old has pain and stiffness of his left leg. His calf is swollen and feels hard. Which vein is likely to be involved?
Correct Answer : D
The key is D. Popliteal vein
Choose a Question
×Choose a Question
×
Trial Access Limit Reached
You’ve reached the limit of free content. Subscribe to continue learning without restrictions.