

Hello,
Dr. Batman
Hello Doctor, Welcome!
Profile
Name: Batman
Email: batman@gotham.com
NEPHROLOGY
(Total Questions - 40)Q.1. A 26 year old mountain biker was rescued after being trapped under heavy rocks for almost 12 hours. His urine is dark and urine is positive for blood on dipstick. His heart rate is 120 bpm and systolic blood pressure is 100 mmHg. Lab results show a creatinine of 35 micromol/L and urea of 15 mmol/L. What is the most appropriate management?
Correct Answer : A
This patient here has attained severe crush injuries which have led to rhabdomyolysis which results from skeletal muscle breakdown, with the release of its contents, one of which is myoglobin into the circulation.
Myoglobin has heme which results in a positive dipstick for blood. Myoglobin is nephrotoxic and can cause a worsening acute kidney injury. It is important to rehydrate the patient to decrease the duration of contact between myoglobin and the kidney tubules.
RHABDOMYOLYSIS :
Rhabdomyolysis results from skeletal muscle breakdown, with the release of its contents into the circulation, including myoglobin, potassium, phosphate, urate, and creatinine kinase (CK).
Aetiology :
• Sudden, severe crush injury
• Status epilepticus
• Severe exertion
Important presentations to remember for the exam :
• Elderly patient with a history of falls followed by long duration on the floor
• Mountain biker rescued from being trapped under heavy rocks for many hours
• Trapped under a fallen wardrobe for several hours
• IV drug user found on the floor not moving for a few days
• Marathon runner who just completed a long-distance run
Two complications you need to remember for rhabdomyolysis :
• Acute kidney injury
• Hyperkalaemia
There is often enough pigment release in the bloodstream to cause nephrotoxicity.
The degree of toxicity is related to the duration of contact of the tubular cells with myoglobin.
This toxicity is compounded by dehydration as well. For example, a person who has run a marathon has both myoglobin release as well as poor kidney perfusion. Both dehydration and release of myoglobin increase the risk of acute kidney injury.
One of the most important complications to recognize for rhabdomyolysis is hyperkalemia and thus rhabdomyolysis is often a medical emergency.
The most important test when there has been a severe crush injury and the rhabdomyolysis is potentially life-threatening is an ECG or potassium level. This implies that you know how a patient with rhabdomyolysis will die.
Acidosis and hyperkalemia can lead to an arrhythmia.
If there are peaked T-waves on the ECG, you will give calcium chloride or calcium gluconate. The best initial test that is specific for rhabdomyolysis is a urinalysis in which you find a dipstick that is positive for blood but in which no red cells are seen.
This is a False +ve dipstick haematuria. This is because myoglobin can react with the reagent on the dipstick and come out as if there were red cells present.
Hemoglobin will do the same thing. The dipstick of the urinalysis cannot distinguish among hemoglobin, myoglobin, and red blood cells. This is because myoglobin has heme in it.
Rhabdomyolysis is confirmed with a markedly elevated serum CPK level. Elevated serum CPK is a biochemical marker of skeletal muscle neurosis. Rhabdomyolysis is associated with a very rapidly rising creatinine level. This is because of both renal failure as well as the massive release of muscle products.
Treatment :
* If there are ECG abnormalities from the hyperkalemia the best initial therapy is calcium chloride or gluconate.
• Intravenous fluid rehydration
• Intravenous sodium bicarbonate
* Alkalinizing the urine with bicarbonate may help prevent the precipitation of the pigment in the tubule
• Dialysis - Only needed in severe cases.
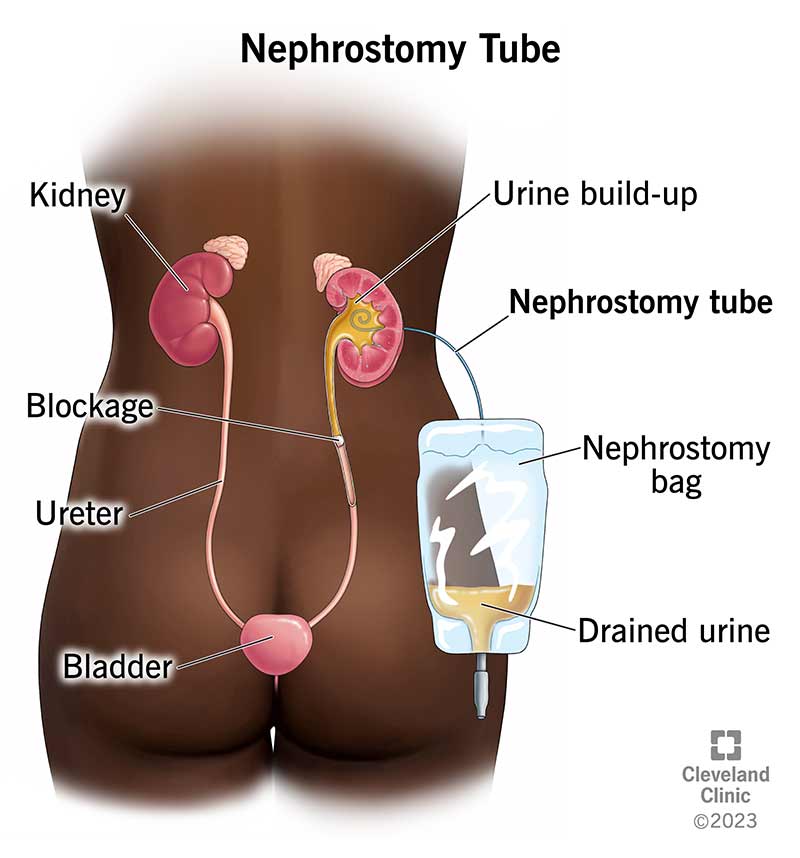
Q.2. A 52 year old known diabetes mellitus presents to the Emergency Department with a sudden onset of pain in the left loin and haematuria. An ultrasound scan shows a 7 mm stone in left lower ureter. Diclofenac was administered for the renal colic pain and nifedipine and prednisolone was prescribed as initial treatment as part of an expulsive therapy. He returns to the emergency department the following day with worsening pain, vomiting and a history of having passed two stones. A repeat ultrasound scan reveals hydronephrosis in the left ureter and the presence of stones. His renal function test indicate an acute kidney injury. He has a heart rate of 100 beats/minute and a temperature of 38.5 C. What is the most appropriate management?
Correct Answer : A
This acute kidney injury and hydronephrosis are indicative of obstructive uropathy. Percutaneous nephrostomy would be the best intervention to temporarily decompress the renal collecting system. ESWL becomes extremely less effective once the stone goes up to 2-3 mm in size. Less than 50% chance of success. This patient has AKI, a very large stone that is obstructive uropathy, and therefore urgent percutaneous nephrostomy is indicated.
Q.3. A 6 year old boy presents to the paediatric outpatient clinic with a two day history of dramatic weight gain and bodily swelling, particularly in his lower limbs. He also had bilaterally puffy eyes two days ago, which he was given some antihistamine syrup for, but they have not improved his symptoms. He is otherwise happy and healthy. His mother reports an uneventful pregnancy and he was delivered via elective Caesarean section at 38 weeks of gestation. He has no medical problems and he is on the 50th centile on all of his growth charts. He takes no chronic medication. The mother reports no significant family history of renal problems. Analysis of the patient’s urine sample was done and is significant for 3+ proteinuria. What is the next best investigation?
Correct Answer : D
The patient’s urinalysis shows significant proteinuria and to confirm the diagnosis of nephrotic syndrome, the next best step would be to check the serum albumin level (which will be low in this case). The patient’s weight gain and limb swelling is due to oedema.
The definition of the nephrotic syndrome includes both massive proteinuria and hypoalbuminemia. The cause of this patient’s proteinuria is most likely to be minimal change disease. The incidence is higher in children between 2 to 5 years of age.
In children, facial swelling is a common presenting feature. However, oedema may progress to involve the whole body.
Minimal change glomerulonephritis nearly always presents as nephrotic syndrome, accounting for the majority of cases in children and about a quarter of cases in adults. Most cases are idiopathic and respond well to steroids.
There is no need to repeat the urine analysis as it already confirms proteinuria.
The next best step would be to check for hypoalbuminemia. Once the diagnosis is confirmed, the child can be referred to the nephrology department for further investigations and treatment.
Q.4. A 23 year old intravenous drug user with known human immunodeficiency virus infection and ongoing alcohol dependence was found on the floor by his friend. According to a neighbour, the last time the patient was seen was two days ago. On examination, he is found to be very confused and disoriented. His blood tests show: Sodium 137 mmol/L Potassium 5.7 mmol/L Urea 45 mmol/L Creatinine 1100 mmol/L What is the best investigation to perform next?
Correct Answer : C
Creatine Kinase is the correct answer as this patient likely has rhabdomyolysis. Creatine kinase is the investigation used to help diagnose this and rhabdomyolysis can result in severe acute kidney injury with life-threatening hyperkalemia if left untreated as well as permanent kidney damage.
Given that the patient had been seen two days ago he may have been lying on the floor for up to two days which is a very high risk of rhabdomyolysis.
Furthermore, as a drug user, he may have used stimulant drugs that would also result in rhabdomyolysis.
Rhabdomyolysis can be the result of muscle ischaemia due to tissue compression in cases of prolonged immobilization, such as comatose situations after an overdose of drugs. A full blood count is incorrect.
Although this may be useful to us in some way, in this case, it is not the single best answer as it does not direct our steps in management greatly help us find a cause for this presentation, or address the main concern in this patient which is the acute kidney injury and rhabdomyolysis.
Blood cultures are incorrect.
The Abdominal ultrasound scan is incorrect. Although this imaging is non-invasive and would potentially give us a picture of the kidneys, it is not entirely necessary as the next step in investigating this patient. It would not help us to diagnose rhabdomyolysis at all.
It would be helpful later on to check for any gross structural damage to the kidney.
Amylase is incorrect as in this case, it would not help further the management or diagnosis in this case.
Amylase is usually used as a blood test when we are suspicious of pancreatitis. In this case, there is no clear story of abdominal pain or vomiting, which are classic as well as common features of pancreatitis.
Q.5. An 18 year old man reports having several episodes of visible haematuria over the last 24 hours. There is no history of abdominal pain or loin pain. These typically seem to occur within a day or two of developing an upper respiratory tract infection. Urine testing by dipstick shows albumin and blood. What is the most likely diagnosis?
Correct Answer : D
IgA nephropathy (Berger's disease)
Features :
• Young male, recurrent episodes of macroscopic haematuria
• Typically usually with an upper respiratory tract infection or, less often, gastroenteritis. Most patients have a history of an upper respiratory tract infection and, either at the onset or within the first 24-48 hours, there is gross haematuria that lasts for less than three days. The urine is red or brown and there may also be loin pain.
• Alternatively, there may be no symptoms but urine shows erythrocytes, casts, and proteinuria.
• It is associated with several other diseases, including Henoch-Schönlein purpura.
• Of those that do not remit, there is a slow progression to ESRD.
IgA nephropathy :
• Develops 1-2 days after URTI
• Main symptom – Haematuria
• Young males
Post-streptococcal glomerulonephritis :
• Develops 1-2 weeks after URTI
• Main symptom – Proteinuria
• Associated with a low complement level.
Q.6. A 27 year old lady was admitted with fever, rigors, and right loin pain. A dipstick urinalysis was positive for blood, leukocyte esterase and nitrites. A midstream specimen of urine (MSU) was sent for culture. She has no medical history of significance. What is the appropriate action?
Correct Answer : B
Patients with suspected acute pyelonephritis should be started with empirical antibiotics immediately. The antibiotic choice depends on local guidelines however ciprofloxacin or co-amoxiclav intravenously would be a good choice here if asked.
Antibiotics can be reviewed or changed after the cultures and sensitivities are available. Good hydration is also advised, however, antibiotics are still a more appropriate action in this scenario.
Maintaining a high urine output helps resolve acute pyelonephritis by flushing the bacteria from the kidney.
ACUTE PYELONEPHRITIS : Pyelonephritis is an inflammation of the kidney and renal pelvis caused by ascending urinary tract infections.
Risk factors - Structural renal abnormalities, including vesicoureteric reflux (VUR)
- Calculi and urinary tract catheterization
- Stents or drainage procedures
- Pregnancy
- Diabetes
- Primary biliary cirrhosis
- Neuropathic bladder
- Prostate enlargement
Presentation :
- Onset is rapid with symptoms appearing over a day or two
- Unilateral or bilateral loin pain, suprapubic pain or back pain
- Fever is variable but can be high enough to produce rigors
- Nausea, vomiting
- Accompanying symptoms suggestive of a lower UTI (frequency, urgency, suprapubic pain, urethral burning, or pain on voiding)
Investigations : Urinalysis to look for blood, protein, leukocyte esterase, and nitrite.
- Midstream specimen of urine (MSU) for microscopy and culture – (this should be done preferably before starting empirical antibiotics).
For children, the collection may need to be a clean catch, catheter, or suprapubic aspiration.
Management :
• Usually requires admission
• Antibiotics.
Empirical antibiotic treatment whilst awaiting culture and sensitivity.
• Pregnant women who do not require admission (unlikely to be asked in the exam). If the patient is being admitted, intravenous antibiotics would be suitable.
Q.7. A 50 year old woman who is newly diagnosed with hypertension complains of urinary frequency and dysuria for the past two weeks. Urinalysis reveals the presence of white blood cells and protein. What is the most appropriate management for her?
Correct Answer : A
This lady has a urinary tract infection. The hypertension given in this stem has no relationship to the management and it is given to throw you off. Trimethoprim would be the most appropriate choice given that it is an antibiotic used to treat UTI.
Q.8. A 32 year old miner was rescued after being trapped under a fallen rock for 4 hours. After applying a bladder catheter, 145-20 ml of reddish brown urine was obtained. He has a systolic blood pressure of 100 mmHg and a pulse rate of 130 beats/minute. What is the most appropriate next management?
Correct Answer : C
The patient developed rhabdomyolysis as he was trapped under a fallen rock for several hours. The reddish brown sometimes referred to as ‘tea-colored’ urine is due to myoglobin in the urine. Due to the danger of acute renal failure, intravenous fluids would be an appropriate option to avoid further renal compromise.
Q.9. A 65 year old diabetic woman is undergoing a coronary angiography. What is the most appropriate measure to prevent contrast induced nephropathy?
Correct Answer : D
Dehydration can increase your risk of contrast-induced nephropathy. Thus, drink fluids to prevent dehydration. IV normal saline can help prevent dehydration as well. The evidence supporting their use is strong.
In practice, 0.9% NaCl 1mL/kg/h for 12h pre- and 12h post-procedure is given to patients.
Q.10. A 56 year old man presents with periorbital and pedal oedema. 24-hour urine shows 8 g of protein and his serum cholesterol is 7 mmol/L. A recent serum creatinine performed showd a level of 258 micromol/L from a baseline of 180 micromol/L. Renal biopsy was performed however, results have not come back yet. What is the most likely cause of his nephrotic syndrome?
Correct Answer : B
Membranous nephropathy is the most common form of idiopathic nephrotic syndrome in this age group.
It has a peak incidence in the 4th to 6th decades of life.
The top 4 causes of the nephrotic syndrome in descending order of frequency in adults:
- Membranous nephropathy
- Minimal change nephropathy
- Systemic lupus erythematosus
- Focal and segmental glomerulosclerosis.
If the stem includes a non-diabetic causation adult or otherwise unspecified like in this stem, with nephrotic syndrome, the answer should always be membranous nephropathy when asked about the likely cause.
MEMBRANOUS NEPHROPATHY :
This occurs when there is a widespread thickening of the glomerular basement membrane.
It is the most common form of idiopathic nephrotic syndrome in adults.
Clinical features :
• Proteinuria associated with the nephrotic syndrome
• Microscopic haematuria
• Hypertension 75% of membranous nephropathy is idiopathic with 25% of them having a secondary cause.
Q.11. A 2 year old boy is brought to the hospital by his mother with the complaints of diarrhoea and vomiting. He was previously fit and well until a few days ago when he was treated with antibiotics by his general practitioner for an upper respiratory tract infection. He no longer has a cough but feels extremely unwell. His observations show that he is tachycardia and tachypnoeic. His recent blood test shows: Sodium 134 mmol/L Potassium 5.9 mmol/L Urea 10.1 mmol/L Creatinine 195 micromol/L. What is the likely diagnosis?
Correct Answer : C
You may be tempted to choose gastroenteritis as an answer to this question. Although gastroenteritis is a viable option here given the patient’s symptoms, remember that prolonged vomiting and diarrhoea cause hypokalaemia and not hyperkalemia.
Acute kidney injury is the correct answer here as can be seen clearly with the lab values.
Whether this child got an acute kidney injury from his previous upper respiratory tract infection, from antibiotic use, or dehydration due to vomiting and diarrhoea remains unknown.
It is worth mentioning that prerenal is the most common cause of acute kidney injury in children and it would usually occur from hypovolaemia.
Q.12. A 32 year old man presents with painless haematuria and flank pain. His blood pressure is 155/98 mmHg. The rest of the physical examination was otherwise unremarkable. What is the most likely diagnosis?
Correct Answer : D
For the examination, scenarios with haematuria + hypertension are almost always polycystic kidney disease (PKD). Questions often ask about screening tests for PKD and give you an option between genetic testing for PKD1 or an ultrasound scan. The answer should always be an ultrasound scan.
Genetic testing for PKD1 is difficult as the gene is large and there are hundreds of described mutations.
USS screening offers good sensitivity and specificity.
Autosomal dominant polycystic kidney disease
Presentation :
- Flank pain
- Haematuria (micro and gross)
- Urinary tract infections (UTIs) and calculi
- Hypertension
- Bilateral kidney enlargement
- Abdominal examination may reveal enlarged and palpable kidneys
Other points:
- Gross haematuria following trauma is a classic presenting feature of ADPKD
- Sometimes present with kidney failure (usually in the fourth to the sixth decade of life)
- May also present as asymptomatic on screening of family members
- Intracranial aneurysm is an important extrarenal manifestation (an important point that is commonly asked)
Note: The other extra-renal manifestations are less commonly asked
Diagnosis: Ultrasound
Treatment : Management of hypertension.
Q.13. A 3 year old child presents to A&E with history of bloody diarrhoea and decreased urination. The mother states that the child developed fever, vomiting, abdominal pain, and diarrhoea that started 5 days ago. On physical examination, the patient appears ill. He is pale and lethargic. Laboratory results show: Haemoglobin 90 g/L Platelets 80 x 109/L There was fragmented red cells on blood film. What is the most likely diagnosis?
Correct Answer : A
Haemolytic uraemic syndrome (HUS) :
HUS consists of a triad of haemolytic anaemia, uraemia, and thrombocytopenia. The anaemia will be intravascular and will have an abnormal blood smear showing schistocytes, helmet cells, and fragmented red cells.
LDH and reticulocyte count will be elevated and the haptoglobin will decrease. 90% are caused by E. coli strain O157. This produces a verotoxin that attacks endothelial cells. Occurs after eating undercooked contaminated meat.
Signs and Symptoms: The classical presenting feature is profuse diarrhoea that turns bloody 1 to 3 days later.
Management :
• Treatment is supportive e.g. Fluids, blood transfusion, and dialysis if required
• Do not give antibiotics to those with possible HUS. The organism may release more toxins as it dies if antibiotics are given which may worsen the disease.
• The indications for plasma exchange in HUS are complicated. As a general rule plasma exchange is reserved for severe cases of HUS not associated with diarrhoea.
Q.14. A 16 year old boy presents to hospital complaining that his urine has been very dark recently resembling tea. He had recently been under “the weather” 2 weeks back and had taken a few days off work with a sore throat and coryzal symptoms. A urine dipstick returns highly positive for blood and protein. He is admitted for supportive management. What is the most likely diagnosis?
Correct Answer : C
Post-streptococcal glomerulonephritis typically occurs 7-14 days following a group A beta-haemolytic Streptococcus infection (usually Streptococcus pyogenes).
It classically follows a streptococcal sore throat but often occurs after an infection elsewhere, e.g. tonsillitis, pharyngitis (commonly), impetigo, otitis media, and cellulitis. It is caused by immune complex (IgG, IgM, and C3) deposition in the glomeruli.
Young children most commonly affected are usually below age 7.
Clinical presentation : Varies from asymptomatic microscopic haematuria through to an acute nephritic syndrome, with frank haematuria, oliguria, proteinuria, oedema, increased blood pressure, and AKI.
Very commonly patients would describe their urine as smoky, cola, or tea-colored urine. This abnormal urine color is from hematuria, red cell casts, and proteinuria.
Investigations :
- Low C3
- Raised anti-streptolysin O titer
- The most accurate test is the renal biopsy showing "humps" on electron microscopy. IgG and C3 will be deposited in the mesangium as subepithelial humps. However, the biopsy is rarely needed as treatment is largely supportive with the vast majority resolving spontaneously.
Q.15. A 24 year old man has just completed a long-distance running event. He becomes very weak afterward and is brought to the emergency department with painful muscles and red-brown urine. Urine is positive for blood on dipstick but without RBC on microscopy. ECG shows a tall T waves, small P waves, and a widened QRS complex. What is the most appropriate initial management?
Correct Answer : D
This man has just finished a run of which he was severely exerted. The skeletal muscle breakdown has resulted in Rhabdomyolysis and thus hyperkalemia. IV calcium gluconate needs to be administered first for cardioprotection as there are already ECG changes from hyperkalaemia.
Q.16. A 2 year old boy has gradual swelling of his face, feet and legs. He feeds poorly but is noted to have gained weight. There is a foamy appearance of the urine. He feels fatigue. What is the most appropriate investigation?
Correct Answer : A
This is a case of nephrotic syndrome which is likely caused by minimal change disease. Minimal change disease has a peak incidence at 2 to 3 years of age. Almost all cases are idiopathic but a small percentage of cases have identifiable causes like NSAIDs, toxins, and infections.
Children with minimal change disease often gain weight, as they are excreting less water in their urine. Testing the renal function is important however in most cases it would be normal (hyponatremia is often observed due to water retention). A 24-hour urine measurement for protein and creatinine clearance is a better answer.
NEPHROTIC SYNDROME :
Triad of:
1. Proteinuria (> 3g/24hr) causing
2. Hypoalbuminaemia (< 30g/L) and
3. Oedema
Causes : Primary glomerulonephritis accounts for around 80% of cases
- minimal change glomerulonephritis
- membranous glomerulonephritis
- focal segmental glomerulosclerosis
- membranoproliferative glomerulonephritis
Systemic disease
- diabetes mellitus
- systemic lupus erythematosus
- amyloidosis
Q.17. A 10 year old boy has been diagnosed with nephrotic syndrome and started on steroids. 5 days later he presents with flank pain, haematuria and fluctuating urea levels. A diagnosis of renal vein thrombosis is made. What is the most likely cause for renal vein thrombosis?
Correct Answer : B
Nephrotic syndrome is the combination of proteinuria, oedema, and hypoalbuminaemia. Not only is albumin lost in the urine, but anti-coagulation factors are also lost such as antithrombin III.
A reduction or deficiency in antithrombin III predisposes patients to venous thromboembolism. Protein C is present in the urine of nephrotic patients and its deficiency can also predispose to venous thromboembolism.
However, plasma levels remain within normal limits and it is not thought to be involved in the development of renal vein thrombosis in these patients.
Treatment of renal vein thrombosis is with anticoagulation. It is unclear why the renal vein is susceptible to thrombosis.
The most common cause of nephrotic syndrome in children is minimal change disease.
Q.18. A 79 year old man has anorexia, urinary frequency, hesitancy, and post-void dribbling. He is also hypertensive, with a blood pressure of 165/110. There are small kidneys on ultrasound and a creatinine of 170 mmol/L. What is the most likely diagnosis leading to his renal dysfunction?
Correct Answer : C
Hypertensive renal disease leads to small, scarred kidneys. This elderly man has anorexia which may suggest prostatic cancer.
However, a large prostate can lead to obstructive nephropathy and hydronephrosis, not small kidneys. Reflux nephropathy leads to dilated renal pelvis and calyces.
Q.19. A 79 year old man found on the floor unconscious by his neighbours. When the paramedics arrived at the scene, he gained consciousness with a GCS of 15/15. His systolic blood pressure with the ambulance crew was 60 mmHg of which the ambulance crew administered 1.5 L of sodium chloride 0.9%. On arrival to the Emergency Department, the was resuscitated further. He gives a history of having severe diarrhoea over the past 2 days. His venous blood gas shows the following: pH 7.18 Base excess – 14 mmol/L Lactate 6.1 His other bloods show: Haemoglobin 118 g/L Urea 16 mmol/L Creatinine 400 micromol/L eGFR 16 CRP 160 mg/L What is the most likely interpretation of his blood gas?
Correct Answer : D
This picture represents metabolic acidosis :
• His pH is low – Acidosis
• His base excess is very low – Metabolic acidosis
Diarrhoea can cause a loss of bicarbonate from the body causing metabolic acidosis. Diarrhea and sepsis would also exacerbate dehydration and hypovolaemia which may produce a pre-renal element of acute renal failure which is represented by the high serum creatinine. In this case, there are many factors which can be seen to contribute to the metabolic acidosis.
• Diarrhoea – loss of bicarbonates
• Septic shock – a build-up of lactic acid
• Renal failure – a build-up of urate
ACUTE KIDNEY INJURY (AKI) :
• Characterised by a decreased renal function which occurs over hours to days
• Measured by serum creatinine or urine output
Remember the 5 most common causes of AKI :
1. Sepsis
2. Major surgery
3. Cardiogenic shock
4. Other causes of hypovolaemia
5. Drugs
Q.20. In chronic renal failure, what is the main cause of vitamin D deficiency?
Correct Answer : B
Patients with kidney disease have reduced activity of the enzyme 1-alpha hydroxylase in the kidneys, which converts 25-hydroxyvitamin D to its more active form, 1, 25-dihydroxyvitamin D, and thus patients with kidney disease have traditionally been given vitamin D replacement with active 1,25-dihydroxyvitamin D or a related analog.
Q.21. A 32 year old woman of 38 weeks gestation complains of feeling unwell with fever, rigors and abdominal pains. The pain was initially located at the lower abdomen and was associated with urinary frequency and dysuria. The pain has now become more generalized specifically radiating to the right loin. She says that she has felt occasional uternine tightening. CTG is reassuring. What is the most likely diagnosis?
Correct Answer : C
Fever, rigor, abdominal pain associated with frequency and dysuria, and radiation to the right loin suggest right-sided pyelonephritis. Acute pyelonephritis is more common in pregnancy.
Q.22. A 29 year old lady was admitted with fever, rigors, loin pain and vomiting. A dipstick urinalysis was positive for blood, leukocyte esterase and nitrites. She has a history of repeated urinary tract infections, but this time she has blood in her urine. What is the most likely diagnosis?
Correct Answer : A
The loin pain is suggestive of acute pyelonephritis. Urinary tract infection is not wrong as acute pyelonephritis is under the category of a urinary tract infection but the more specific answer would be acute pyelonephritis. Many doctors would have answered chronic pyelonephritis because of the history of repeated urinary tract infections. However, chronic pyelonephritis usually has no active infection. They may present with symptoms secondary to renal failure. Diagnosis is often from incidental findings during general investigation.
Q.23. A 6 year old boy is brought to the emergency department by his mother because of swelling on his legs that has been worsening in the last two days. The swelling is also present in the scrotum and around his eyes. He is generally tired and his urine is noted to be frothy. Renal biopsy report states no abnormalities can be seen on light microscopy, however, electron microscopy reveals abnormal podocytes (fused). What is the most likely diagnosis?
Correct Answer : B
The phrase “electron microscopy shows fusion of podocytes“ is key. This tells you that it can be nothing else but minimal change in disease.
These questions would likely give a scenario similar to this where a child is having symptoms of swelling or proteinuria and a renal biopsy shows a fusion of podocytes on electron microscopy.
Minimal change disease nearly always presents as nephrotic syndrome, accounting for 75% of cases in children and 25% in adults.
The majority of cases are idiopathic
Features :
- Nephrotic syndrome
- Normotension
- Hypertension is rare
- Renal biopsy: electron microscopy shows fusion of podocytes
Management :
- Majority of cases (80%) are steroid responsive
- Cyclophosphamide is the next step for steroid-resistant cases.
Q.24. A 9 year old boy is brought in by his parents with bilateral periorbital oedema, ankle swelling and an increase in body weight. What is the most likely diagnosis?
Correct Answer : C
This patient most likely has a nephrotic syndrome :
• Proteinuria
• Hypoalbuminaemia
• Oedema
The most likely diagnosis is minimal change disease.
The peak incidence is around 3-4 years of age. However, it can occur in older children. It is steroid-responsive in the majority of cases, however a small number of patients require cyclophosphamide.
The diagnosis of minimal change disease can be made on clinical and biochemical grounds alone.
However, a renal biopsy can be performed to demonstrate podocyte fusion and deformity on electron microscopy. IgA glomerulonephritis causes nephritis and typically occurs a few days after an upper respiratory tract infection.
Q.25. A 24 year old male was trying to move his wardrobe when it fell on his thigh. His two legs were trapped underneath it for several hours before someone was able to help him get out. When he was seen in the ED his urine was dark and dipstick was positive for blood. His heart rate is 115 bpm and his systolic blood pressure is 100 mmHg. Lab results show a creatinine of 320 micromol/L and urea of 13 mmol/L. What is the most likely cause of his renal failures?
Correct Answer : D
The trauma to his muscles and being left there for several hours has led to muscle breakdown which would release myoglobins causing an acute kidney injury which can be seen by the raised creatinine and urea in this stem.
Q.26. A 79 year old man is brought in by ambulance to the Emergency Department as he is feeling unwell and short of breath. His arterial blood gas shows the following: pH 7.15 pCO2 2.2 kpa PO2 12 kpa Base excess -16 mmol/L Hisother bloods show: Urea 15 mmol/L Creatinine 350 micromol/L What is the most likely interpretation of his arterial blood gas?
Correct Answer : C
Metabolic acidosis with partial respiratory compensation would be the best answer here. As this is not present, pick metabolic acidosis.
• His pH is low – Acidosis
• His base excess is very low – Metabolic acidosis
• His pCO2 is low – Because of respiratory compensation the lungs are attempting to clear out carbon dioxide.
One of the causes of a dyspnoeic patient like in this stem is respiratory compensation for metabolic acidosis.
This is usually seen in a patient who is DKA or a patient with salicylate overdose which the stem may not always reveal.
Q.27. A 75 year old female presents to A&E with the history of a fall. On further questioning, it is revealed that she has had a two year history of frequent falls, the cause of which she attributes to being clumsier in her old age. On examination, she appears to be confused and has a three hour history of nausea and vomiting. She has decreased skin turgor and is found to be oliguric. Her serum lab values are as follows: Urea: 15 mmol/L Creatinine: 210 micromol/L Creatine kinase: 21223 U/L What is the most likely reason for her increased creatine kinase levels?
Correct Answer : A
The answer that best fits in with this patient’s signs and symptoms is rhabdomyolysis. She has an acute kidney injury secondary to rhabdomyolysis which was caused by her history of frequent falls.
The clincher in this stem is the markedly raised serum creatinine kinase, which, in rhabdomyolysis, is often raised to over 10,000. One must remember that you do not need to have a crushing injury for rhabdomyolysis to occur.
It can also occur after a fall if left for a long period on the floor which could also cause muscle breakdown.
There is no history in this stem of being on the floor for a long duration of time, but one would have to assume so as there is not a better option given as an answer.
Some may argue that dermatomyositis may also cause a raised creatinine kinase that is sometimes 50 times more than normal and she could have fallen frequently due to proximal muscle weakness.
However, this stem does not include any skin manifestations like Gottron’s papules or heliotrope rash which are often seen in stems where the answer would be dermatomyositis.
Furthermore, the examiners would always consider which is a more important diagnosis NOT to miss. If you miss a diagnosis of dermatomyositis in A&E, no one will penalize you. But if you miss a diagnosis of rhabdomyolysis which is a medical emergency and life-threatening, a clinical incident would be filed.
Q.28. A 34 year old woman with diabetes mellitus is undergoing a contrast radiography. What is the most appropriate measure that should be taken to prevent renal damage with contrast dye?
Correct Answer : B
Please see Q-9
Q.29. A 65 year old man is being treated for abdominal sepsis with antibiotics and intravenous fluids. After some time repeat blood tests were performed to check the progress. Blood tests showed: Sodium 127 mmol/L Potassium 3.7 mmol/L Creatinine 80 mmol/L Urea 4.3 mmol/L What is most likely cause of these blood test results?
Correct Answer : D
Iatrogenic is the correct answer as these results are likely due to too much of an inappropriate fluid being prescribed such as 5% dextrose.
Hypertension is incorrect as high blood pressure does not cause hyponatremia. Hypernatraemia can result in a raised blood pressure in certain endocrine problems.
Sepsis is incorrect as this alone is not likely to cause low sodium. Certain infections such as atypical respiratory infections like legionella can result in hyponatraemia. In this question, they explicitly state this is an abdominal sepsis.
Liver failure is not correct as there is no indication in this scenario of any liver symptoms.
Although the patient has abdominal sepsis, which is usually biliary sepsis, there is no mention of any signs of liver disease such as jaundice, and there are no blood test results that demonstrate deranged liver function.
Q.30. A 34 year old primigravida who is now 16 weeks gestation attends the antenatal clinic for a routine check up. She has a blood pressure of 160/100 mmHg. She has a history of repeated childhood urinary tract infections. What is the most likely cause of her high blood pressure?
Correct Answer : C
Repeated urinary tract infections in childhood can lead to renal scarring and chronic pyelonephritis which results in hypertension.
Chronic pyelonephritis : This describes renal scarring which may or may not be related to previous UTI. It is a radiological, functional, or pathological diagnosis or description.
Causes :
• Renal scarring due to previous infection
• Long-term effects of VUR, with or without superimposed infection
• A child with VUR, particularly where there is reflux of infected urine, will develop reflux nephropathy (which, if bilateral, may cause renal impairment or renal failure). If the child’s kidneys are examined radiologically, the radiologist will describe the appearance as those of ‘chronic pyelonephritis’.
• An adult may also develop radiological features of chronic pyelonephritis due to the presence of reflux combined with high bladder pressures, again particularly where the urine is infected.
Presentation :
- Patients may be asymptomatic or present with symptoms secondary to renal failure.
Diagnosis is often from incidental findings during general investigation.
- There is usually no active infection.
- Renal ultrasound may show small kidneys with a thin cortex
- Intravenous pyelogram (IVP) may show small kidneys, ureteric and caliceal dilatation/blunting with cortical scarring
- Micturating cystourethrogram (MCUG) may help to identify reflux.
- Technetium-99m , Tc-DMSA scan is the most sensitive for demonstration of renal scars.
Management :
• Aim to investigate and treat any infection, prevent further UTI, and monitor and optimize renal function.
• Blood pressure should be controlled to slow the progression of chronic kidney disease. Ideally using angiotensin-converting enzyme (ACE) inhibitors
• Severe underlying VUR diagnosed in children may require antibiotics prophylactically until puberty or until the reflux resolves.
Q.31. A 58 year old man complains of tiredness, lethargy, nausea and severe itching which is worse after a hot bath and at night. His skin appears pale and dry with increased skin pigmentation and numerous scratch marks. Peripheral oedema is noted on examination. What is the most likely diagnosis?
Correct Answer : A
The signs and symptoms point towards chronic renal failure.
Uraemic pruritus also known as chronic kidney disease-associated pruritus refers to excessive urea in the blood and occurs when both kidneys fail to work sufficiently. It is a common feature of end-stage renal disease and has been seen to affect one-third of patients on dialysis.
Q.32. A 45 year old known hypertensive man presents with tiredness, lethargy, fluid retention and proteinuria. His albumin levels are low. What is the most definitive diagnostic test?
Correct Answer : D
This patient is presenting with nephrotic syndrome. The definitive test to do is a renal biopsy as this would provide us with the aetiology.
Q.33. A 35 year old woman presents to her general practitioner for a routine medical check-up. Upon questioning, it was revealed that she has no significant medical history of note. She is on no chronic medication and has no significant family history. The patient does not drink alcohol and is extremely careful about her health. She has had two successful pregnancies carried to term and both her children are healthy and well. Dipstick urinalysis revealed the presence of 1+ protein. What is the most appropriate next step in the management of this patient?
Correct Answer : A
A dipstick analysis is the most common test in the outpatient setting to evaluate urine protein concentration as well as other markers of renal disease.
Q.34. A 35 year old lady presents with a 12 day history of haemoptysis, and 24 hour history of haematuria. In last 24 hours she has become increasingly breathless and oliguric. A chest X-ray shows patchy interstitial infiltration predominantly affecting both lower zones. Her blood tests show: Haemoglobin 98 g/L Serum urea 9.5 mmol/L Serum creatinine 393 micromol/L Sodium 136 mmol/L Potassium 5.9 mmol/L What is the most appropriate investigation?
Correct Answer : B
The likely diagnosis here is Goodpasture syndrome. The blood reflects an acute kidney injury. The slightly lower haemoglobin levels can be explained by persistent intrapulmonary bleeding. Anti-GBM antibodies are diagnostic.
Goodpasture syndrome :
- Goodpasture's syndrome is the coexistence of acute glomerulonephritis and pulmonary alveolar haemorrhage
Presentation :
• Typically presents as acute kidney injury caused by a rapidly progressive glomerulonephritis, accompanied by pulmonary haemorrhage that may be life-threatening
• Lung involvement is characterized by haemoptysis, cough, and shortness of breath. Anti-glomerular basement membrane antibodies antibodies are diagnostic. Remember: The best initial test to confirm the diagnosis is anti-GBM antibodies.
The SINGLE most accurate test is a lung or kidney biopsy.
Management for Goodpasture syndrome is highly unlikely to be asked given that Goodpasture's syndrome is an uncommon disease.
But one should remember the principles of management:
- Plasmapheresis (plasma exchange) to remove circulating antibodies
- Treat with immunosuppressant medications to prevent further production of antibodies.
Q.35. A 4 year old child presents with swelling. Periorbital oedema, lower limb oedema and oedema of the genitals were noted on examination. A urine dipstick shows proteinuria. He has a normal renal function, normal blood pressure, normal complement levels. What is the most likely diagnosis?
Correct Answer : C
Please see Q-23
Q.36. A 65 year old woman with diabetes, and hypertension underwent a total right hip replacement. She had massive haemorrhage during the operation and was given 8 units of packed red blood cells. The blood pressure dropped to 60/40 mmHg for about two hours before it was corrected with intravenous fluids and blood transfusions. Two days after the surgery, her blood results show: Serum creatinine level rose to 255 micromol/L Potassium 5.1 mmol/L She had a normal kidney function prior to the surgery. What is the most likely diagnosis?
Correct Answer : A
Acute tubular necrosis (ATN) can occur after a prolonged ischaemic event which likely took place here as there was a massive haemorrhage and a hypotensive shock. This is supported by the increased creatinine. Acute tubular necrosis is the most common renal cause of acute kidney injury.
Other stems may include a history of nephrotoxins such as aminoglycosides, radiological contrast, and myoglobinuria in rhabdomyolysis.
Q.37. A 42 year old woman with a past medical history of severe headache treated in the emergency department presents with signs and symptoms of renal failure. She has been seen by her GP for hypertension and loin pain with outpatient investigation pending. What investigation is most likely to lead to a diagnosis?
Correct Answer : B
The initial symptoms of headache and hypertension in this scenario would make you consider renal artery stenosis. However, in addition to the loin pain and features of renal failure, the diagnosis of autosomal dominant polycystic kidney disease is more likely.
This is best diagnosed using ultrasound of the kidneys, ureters & bladder. Questions often ask about screening tests for PKD and give you an option between genetic testing for PKD1 or an ultrasound scan.
The answer should always be an ultrasound scan. Genetic testing for PKD1 is difficult as the gene is large and there are hundreds of described mutations. USS screening offers good sensitivity and specificity.
Autosomal dominant polycystic kidney disease :
Presentation :
- Flank pain
- Haematuria (micro and gross)
- Urinary tract infections (UTIs) and calculi
- Hypertension
- Bilateral kidney enlargement
- Abdominal examination may reveal enlarged and palpable kidneys
- Gross haematuria following trauma is a classic presenting feature of ADPKD
- Sometimes presents with kidney failure
- May also present as asymptomatic on screening of family members
- Intracranial aneurysm is an important extrarenal manifestation (an important point that is commonly asked)
Diagnosis: Ultrasound
Treatment : Management of hypertension.
Q.38. A 45 year old man with renal cell carcinoma recently underwent a left nephrectomy two weeks ago. He presents feeling unwell with a temperature of 38.3°C and he has not been able to pass urine for a day. An ultrasound scan was performed which shows a 9 mm stone in the right lower ureter with dilatation of the pelvicaliceal system. What is the best initial management for this man?
Correct Answer : C
The patient has a single-function kidney and an obstructive uropathy. It is imperative to prevent damage to the remaining kidney by performing a percutaneous nephrostomy to temporarily decompress the renal collecting system.
Q.39. A 31 year old woman has urinary frequency, pain on voiding and back pain. Her urine is cloudy with an offensive smell. She has a temperature of 38.6 C. Her urinalysis showed leukocytes 2+ and nitrates +. Her midstream urine sample was sent off for microscopy and culture. What is the most likely causative organism?
Correct Answer : A
The patient has a urinary tract infection. She displays lower urinary tract symptoms like urinary frequency, pain on voiding) and symptoms of pyelonephritis (back pain and fever.
Escherichia coli causes around 80% of urinary tract infections.
Q.40. A 57 year old male presents to Accident & Emergency with the complaint of weakness and confusion. His wife, who accompanies him, gives a history of her husband first complaining of a loss of sensation in his fingers and muscle cramps which has now deteriorated to this. The patient’s past medical history is significant for chronic kidney disease stage 4, diagnosed two years ago and non-insulin dependent diabetes mellitus which was diagnosed seven years ago. He currently takes metformin and enalapril. Blood tests were carried out and the results are as follows: Sodium 138 mmol/L (135-145 mmol/L) Potassium 5.9 mmol/L (3.5-5.0 mmol/L) Calcium (Total) 1.8 mmol/L (2.1-2.6 mmol/L) Phosphate 2.9 mmol/L (0.8-1.4 mmol/L) Parathyroid hormone (PTH) 4.2 pmol/L (0.8-8.5 pmol/L) Alkaline phosphatase (ALP) 45 U/L (30-150 U/L) What is the most likely cause that can account for the patient’s presentation?
Correct Answer : C
His symptoms are the result of hypocalcemia. Unfortunately, hypocalcemia is not one of the options as that would be too easy. The patient has chronic kidney disease (CKD) which may have resulted from years of having poor glycaemic control leading to diabetic nephropathy.
Chronic kidney disease results in a decrease in the conversion of 25-hydroxyvitamin D to its active form 1, 25 dihydroxyvitamin D, especially when the glomerular filtration rate (GFR) falls below 30 mL/min.
This results in low calcium absorption which also increases parathyroid hormone.
Even though this patient has hyperphosphataemia as seen by the given lab results, it is not the correct answer because an isolated increase in serum phosphate level rarely presents with any outward signs or symptoms.
Choose a Question
×Choose a Question
×
Trial Access Limit Reached
You’ve reached the limit of free content. Subscribe to continue learning without restrictions.