

Hello,
Dr. Batman
Hello Doctor, Welcome!
Profile
Name: Batman
Email: batman@gotham.com
NEUROLOGY
(Total Questions - 310)Q.1. A 58 year old man has visual hallucinations of animals walking around his room. He is amused by them but is conscious that they are not real. He is noted to have functioning levels of awareness and attention and a decline in problem solving ability. Signs of mild parkinsonism are also seen. What is the most likely diagnosis?
Correct Answer : C
The most important features of Lewy body dementia that differentiate it from the other forms of dementia are the:
• Visual hallucinations
• Fluctuating course with lucid intervals
• Signs of mild Parkinsonism
Typical presentation of Lewy body dementia :
• Dementia is usually the presenting feature, with memory loss, decline in problem-solving ability, and spatial awareness difficulties.
• Characteristically there are fluctuating levels of awareness and attention.
• Signs of mild Parkinsonism (tremor, rigidity, poverty of facial expression, festinating gait). Falls frequently occur.
• Visual hallucinations and illusions. 
Q.2. A 67 year old female who was initially admitted to hospital for hip replacement surgery is incidentally found to be confused and drowsy by the ward nurse. The ward nurse also discovers that she has been receiving a continuous infusion of 5% dextrose in sodium chloride 0.45% intravenously since her admission into hospital. The fluid was immediately stopped following this discovery and bloods were taken for a test. Laboratory values show: Sodium 120 mmol/L Potassium 4.8 mmol/L Urea 6.2 mmol/L Creatinine 89 micromol/L Bicarbonate 23 mmol/L Chloride 100 mmol/L What is the most likely cause of this patient’s symptoms?
Correct Answer : B
This patient has hyponatremia leading to cerebral oedema. Cerebral oedema is defined as an excess in the accumulation of fluid in the intracellular or extracellular spaces of the brain there are various causes for this phenomenon, but there are typically four types that can be seen in clinical practice.
The important type to concentrate on for this question is the osmotic type. When plasma is diluted, such as in hyponatremia states, it creates an abnormal pressure gradient between the brain’s internal environment and the serum. This causes the movement of water into the brain. This patient has clear hyponatremia as evidenced by her lab values.
An important cause of hyponatremia is high blood sugar and iatrogenic administration of a hypotonic solution. This patient has been receiving a hypotonic solution and 5% of intravenous dextrose for an extended period. This would naturally increase her blood glucose levels and dilute her intracellular volume leading to hyponatremia. For this reason, sodium chloride 0.9% is usually used instead of hypotonic solutions.
Osmotic shrinkage of the brain describes the result of osmotherapy whereby the volume of intracranial fluid is reduced by shifting fluid out of the brain and into the serum. An example of this type of therapy is administering intravenous mannitol to reduce intracranial pressure. This answer is incorrect as it is the opposite of what the question asks for.
Cerebral demyelination describes any condition that causes the myelin sheath of neurons to become damaged. Although a presenting symptom of demyelination is weakness, this answer is not correct since this patient does not present with the host of signs and symptoms that can be seen in demyelinating diseases which can be anything from diplopia to speech problems.
A common iatrogenic cause of cerebral demyelination is central pontine myelinolysis which is caused by rapid correction of low blood sodium levels. Cytotoxicity is incorrect since the stem gives no clue as to any cytotoxic drug that this patient might have taken. An important cytotoxic drug to remember for the exam is isoniazid, which can lead to cerebral oedema.
Reye’s syndrome describes a rapidly progressive encephalopathy that usually presents with liver toxicity, personality changes, confusion, and even seizures. The cause is unknown, but viral infections are thought to play a role. This answer is incorrect since no clue in the stem alludes to the patient having had a viral infection nor are her liver function test results included .
Q.3. A 50 year old man, known case of hypertension and deep vein thrombosis, presents to the Emergency Department with a sudden onset of vision loss in his right eye. It is painless and lasted for approximately 5 minutes. He describes the vision loss as a ‘black curtain coming down’. On examination, there is a bruit on his neck. What is the most likely condition?
Correct Answer : C
Remember to focus on the causes of unilateral vision loss. Know how to differentiate all the above options. The bruit in the neck is the examiner’s way of telling you that this man has atherosclerosis which is a risk factor for amaurosis fugax.
For amaurosis fugax, this is a classic case stem: sudden, painless, unilateral vision loss and description of a “black curtain coming down”.
Retinal vein thrombosis and retinal artery occlusion present as painless unilateral vision loss but their duration would be much longer if not permanent.
Optic neuritis would have clues in the stem of multiple sclerosis. Acute angle glaucoma would produce a painful vision loss and keywords such as “haloes” would be seen.
Amaurosis Fugax :
• Painless transient monocular visual loss (i.e. loss of vision in one eye that is not permanent)
• It is indicative of retinal ischaemia, usually associated with emboli or stenosis of the ipsilateral carotid artery
Presentation:
• Sudden, unilateral vision loss; “black curtain coming down”
• Duration: 5-15 minutes; resolves within < 24 hours
• Associated with stroke or transient ischaemic attack (TIA) and its risk factors (i.e. hypertension, atherosclerosis)
• Has an association with giant cell arteritis.
Q.4. A 43 year old smoker presents with double vision. She tires easily, has difficulty climbing stairs, and reaching for items on shelves. On examination, reflexes are absent but elicited after exercise. The power in shoulder abduction after repeated testing is 4+/5 from 3/5. What is the most likely pathology associated with this patient’s diagnosis?
Correct Answer : B
This is a diagnosis of Lambert-Eaton syndrome.
A key difference from myasthenia gravis is that on examination the patient has increased strength on repetition of power. It is also a paraneoplastic disorder closely associated with small-cell lung cancer.
Because Lambert-Eaton and myasthenia gravis present similarly, the case stem usually would provide you with an investigation or examination clue, including autoantibodies and EMG results.
Note that thyrotoxicosis is associated with myasthenia gravis, not Lambert-Eaton.
Lambert-Eaton syndrome :
- Young, female patients; mostly autoimmune
- Proximal weakness at the pelvic girdle/shoulder girdle
- Weakness improves with exercise as well as reflexes
- Cranial nerve involvement: dysphagia, dysarthria, ptosis, diplopia
Diagnosis:
- EMG: decreased amplitude in CMAP after a single supramaximal stimulus but increases after exercise
- Edrophonium test: may be positive but not as prominent as in myasthenia gravis
- Look for tumor: CT/MRI of chest, abdomen, pelvis + tumor markers
Treatment:
- Treat tumor – first line
- Consider methylprednisolone and IV immunoglobulin.
Q.5. A 45 year old chronic alcoholic presents to A&E with an ataxic gait, hallucinations and is confused. He is given chlordiazepoxide. What is the most appropriate medication to be given with chlordiazepoxide?
Correct Answer : B
This man is suffering from Wernicke’s encephalopathy.
Wernicke's encephalopathy is a neuropsychiatric disorder caused by thiamine deficiency which is most commonly seen in alcoholics.
A classic triad of confusion, ophthalmoplegia, and ataxia may occur. Treatment is with urgent replacement of thiamine If not treated Korsakoff's syndrome may develop as well.
This is termed Wernicke-Korsakoff syndrome and is characterized by the addition of Antero- and retrograde amnesia and confabulation in addition to the above classic triad.
Wernicke’s Encephalopathy:
1. Confusion
2. Ataxia
3. Ophthalmoplegia
Q.6. A 42 year old lady presents with a history of double vision, ptosis and facial numbness. Which anatomical site is the most likely to be affected?
Correct Answer : D
A brainstem lesion makes the most sense here as the oculomotor nerve arises from the anterior aspect of the mesencephalon (midbrain) while the trigeminal nerve arises from the pons. The involvement of the oculomotor nerve could explain the double vision and the involvement of the trigeminal nerve explains the facial numbness.
Q.7. A 25 year old woman presents with a severe headache. She had migraines for the last 14 years but has been symptom free for the last year. There are no other neurological signs. She has no other medical history of note. Her observations are stable. What is the most appropriate investigation for this woman?
Correct Answer : A
This young lady is likely having a recurrence of her migraine. It is not stated in the stem whether the headache is of a similar type to her previous migraines but one can assume given there are no neurological signs and no mention of neck stiffness or photophobia.
Since this is likely a migraine, no further investigations are required. If there were signs of neck stiffness or photophobia or if the headache was described as the worst headache of her life, obtaining a CT scan of the head would be the choice to rule out a subarachnoid haemorrhage.
Q.8. A 36 year old woman presents to clinic with intermittent episodes of dizziness that lasts 1 day each time for the past 6 months. Recently, she has experienced ringing and increased pressure in her eres. Her husband noticed that she has had to increase the volume of her television. MRI head is normal. What is the most likely diagnosis?
Correct Answer : B
This is a classic case of Meniere’s disease.
All four clues are present: dizziness, tinnitus, deafness, and increased feeling of pressure in the ear.
Know how to differentiate between Meniere’s with options A to C. These topics frequently appear on the neurology component of the exam.
Note that option B is ruled out due to the normal MRI.
In option C, the case would need to give a history of bacterial or viral infection.
In option D, there would be other manifestations, such as weakness or paresthesia of the limbs.
Meniere’s disease :
• Dizziness, tinnitus, deafness, increased feeling of pressure in the ear. Note: Vertigo is usually the prominent symptom
• Episodes last minutes to hours
• MRI is normal
• Usually a female >> male ; 20-60 years old
• Typically symptoms are unilateral but bilateral symptoms may develop after a number of years
Treatment:
• Acute attacks: Buccal or intramuscular prochlorperazine. Admission is sometimes required.
Q.9. An 81 year old man is brought into clinic by his son who is concerned that his father doesn’t seem to be himself. His wife died 3 years ago and has been depressed since. The son notes that his father has become increasingly forgetful, leaving taps running or the stove on when not in use. At times, he cannot articulate what he wants to say and is easily confused. CT brain reveals mild, diffuse cortical atrophy. Which of the following is the most likely medication to be started first?
Correct Answer : C
Alzheimer’s disease is a frequent neurology topic for exam. The main clues usually have an elderly patient undergoing a memory change with some inability to perform day-to-day tasks.
Depending on the severity of the patient, they may have language deficits, executive dysfunction, and cortical atrophy in CT brain.
Acetylcholinesterase inhibitors donepezil, galantamine, and rivastigmine are the first line. Memantine is the second line for severe cases.
This patient is not suffering from hallucinations; therefore, options C and D are ruled out.
While the patient does have depression and would be placed on antidepressants, amitriptyline is contraindicated as it has anticholinergic side effects.
Q.10. A 41 year old women presents to clinic with vertigo, vomiting, and a feeling of aural fullness. The attacks of vertigo can last for several hours. She also states that she has difficulty hearing. She had a similar attack last year. Recently, she has experienced ringing in her ears. MRI scan was done and was found to be normal. What is the most likely diagnosis?
Correct Answer : D
This is a classic case of Meniere’s disease. All four clues are present: dizziness, tinnitus, deafness, and increased feeling of pressure in the ear. It is important to remember that in Meniere’s disease, the attacks can last for several hours at a time, which differentiates it from benign paroxysmal positional vertigo.
Q.11. A 55 year old man presents to clinic with shortness of breath and increased daytime sleepiness. He drinks 25 units of alcohol weekly. On examination, his BMI is 35 kg/m2, blood pressure is 150/70 mmHg, and respiratory exam was normal. His wife complains that he snores loudly at night. What is the most appropriate investigation likely to confirm his diagnosis?
Correct Answer : A
This is a diagnosis of obstructive sleep apnoea syndrome. This topic would overlap between neurology and respiratory medicine.
The typical clues: a middle-aged to elderly male who works at the office, obese, with a history of hypertension and/or diabetes, and “snoring loudly at night”.
The initial test is pulse oximetry but the definitive investigation is polysomnography (gold standard).
Multiple sleep latency test is the definitive investigation for narcolepsy.
Obstructive sleep apnoea syndrome :
- Middle-aged to elderly male
- Increased daytime sleepiness, fatigue, sleep disruption
- Snoring loudly at night
- Associated with hypertension, diabetes, obesity
Diagnosis:
- Pulse oximetry, overnight study of breathing pattern (initial investigation)
- Polysomnography (gold standard)
Treatment:
- Conservative: weight loss and reduced alcohol consumption
- Continuous positive airway pressure (CPAP).
Q.12. A 58 year old man has a progressively worsening headache and confusion. He had a fall three days ago after slipping and hitting his head in the garden. He has a history of alcohol abuse. What is the most appropriate investigation?
Correct Answer : A
The likely cause of his confusion and worsening headache is a subdural haemorrhage. A CT scan is diagnostic.
Subdural haematoma may be acute or chronic. In chronic subdural haematoma, symptoms may not be apparent for several days or weeks. Symptoms of subdural haematomas are fluctuating levels of consciousness, ± insidious physical or intellectual slowing, sleepiness, headache, personality change, and unsteadiness.
Chronic subdural haematoma occurs in very old or severe alcoholics. A shrunken brain is rattled around the head by minor trauma, tearing venous sinuses. Over several days or weeks, mental function deteriorates as haematoma forms.
CT scan is diagnostic, and surgical evacuation provides a dramatic cure. Remember, chronic subdural haematoma usually presents as an elderly, on anticoagulation, or an alcoholic who may have a history of falls. Slow onset of symptoms compared to epidural haematoma.
DIFFERENTIATING TYPES OF TRAUMATIC BRAIN INJURY :
Extradural haematoma:
• Often associated with skull fracture and middle meningeal artery injury
• Lucid intervals (Patient goes back to doing what he was doing before falling unconscious again)
Subdural haematoma:
Chronic Subdural haematoma :
• Usually elderly, on anticoagulation or alcoholic
• History of minor fall with minor head injury
• Slow onset of symptoms compared to epidural haematoma
Acute Subdural haematoma :
• The probable reason is that it is difficult to differentiate from epidural as both have lucid intervals
• Think bigger trauma. Sicker patient
• Patient is barely awake during the lucid intervals In reality, we do not rely on clinical features to differentiate epidural haematoma from acute subdural haematoma because both of them will get a CT scan!
Subarachnoid haemorrhage:
• Aneurysm formation is the most common aetiology
• Usually spontaneously in the context of a ruptured cerebral aneurysm but may be seen in association with other injuries when a patient has sustained a traumatic brain injury
• Association with polycystic kidney disease, Ehlers-Danlos syndrome, and other connective tissue disease
• Hallmark – THUNDERCLAP HEADACHE
• Meningeal irritation (neck stiffness, photophobia).
Q.13. A 69 year old man presented to clinic with worsening balance and difficulty walking over the past year. Recently, he has been prone to falling more frequently and his wife notes he forgets to turn off the stove or water taps. He has also started to have urinary urgency and incontinence. On examination he is walking with a cane and has difficulty turning. What is the most likely diagnosis?
Correct Answer : C
This is a classic presentation: Gait disturbance, sphincter compromise, and dementia.
NPH has a much slower progressive memory loss than Alzheimer’s.
Normal pressure hydrocephalus :
• TRIAD: gait disturbance, urinary incontinence, cognitive dysfunction
• Most common in elderly
• CT / MRI brain: enlarged lateral and third ventricles
Diagnosis:
• Clinical diagnosis with CT/MRI brain signs of enlarged lateral and third ventricles
Treatment:
• Cerebrospinal fluid (CSF) shunting: ventriculoperitoneal, ventriculopleural, or ventriculoatrial.
Q.14. A 66 year old patient wakes up with slurred speech and right sided weakness. He is brought to the hospital by his wife. A computed tomography was ordered and shows a cerebral infarction. What is the most appropriate treatment to be given?
Correct Answer : B
The answer here is aspirin 300 mg. The history and examination are convincing for a stroke. Before any treatment can happen we need to exclude a haemorrhagic stroke with the help of imaging. This was done in this question which showed an ischaemic stroke.
The other options are less likely to be the appropriate next course of action.
The window period to administer alteplase is 4.5 hours from the onset of stroke symptoms. If we cannot be certain of this period, we cannot proceed to give alteplase. Firstly, there was no time given in the stem. Secondly, the patient woke up to the symptoms of a stroke. The ischaemic event could have happened anytime during the night.
Warfarin should not be started until brain imaging has excluded haemorrhage, and usually not until 14 days have passed from the onset of an ischaemic stroke. Note that alteplase is preferred over streptokinase.
So streptokinase is rarely the right answer.
Statins need to be offered but this is not the most appropriate next course of action. There is no urgency in giving statins.
Q.15. A 26 year old man was found on the street to be unsteady and drunk by police. On admission to Emergency, he had a sudden onset of headache with severe intensity. The headache is localized to his occipital area and is continuous. On examination, his GCS is 15/15, afebrile and no focal neurological signs. What is the most likely diagnosis?
Correct Answer : C
Note for the exam, the keywords for subarachnoid haemorrhage (SAH) are “worst headache of my life”, “headache of severe intensity”, “thunderclap headache”, “sudden onset”, occipital”. The other main clue in this stem is the patient was found drunk. Excess alcohol consumption is one main risk factors leading to SAH.
SUBARACHNOID HEMORRHAGE :
Usually the result of bleeding from a berry aneurysm in the Circle of Willis
• Sudden and severe occipital headache described as the “worst headache of my life” or “thunderclap headache”
• Neck stiffness or pain
• Vomiting, collapse, seizures
Associations :
• Hypertension
• Polycystic kidney disease. Berry aneurysms are found in 10% of patients with autosomal dominant adult polycystic kidney disease
• Ehlers Danlos syndrome
Diagnosis :
• CT brain
• Lumbar puncture : The CSF of a lumbar puncture bloody then xanthochromic (bilirubin).
Q.16. A 68 year old man had a fall down the stairs. His daughter has brought him into the emergency department where he was having lucid intervals. Shortly after admission he becomes unconscious. What is the most likely vessel affected?
Correct Answer : D
Lucid intervals followed by unconsciousness are typical for an epidural haemorrhage in which the middle meningeal artery is involved.
Extradural (epidural) haematoma often associated with skull fracture and middle meningeal artery injury. Involves arterial blood.
Features :
• Features of raised intracranial pressure
• Patients may exhibit a lucid interval
Management : Surgical procedure: Burr hole followed by craniotomy and evacuation of the haematoma.
Q.17. A 65 year old female patient has become increasingly distressed. She cries all the time and has been forgetting to lock her doors at night and turn off the stove after she has used it. She is forgetful, having forgotten her son’s birthday this year, which she has never done before. She also gets lost when she goes out, and has difficulty in finding her way back home. On occasion she puts her house keys in the microwave, and she does not appear to know how to use it to cook food anymore. She also has a prominent impairment of recent memory but has an intact immediate recall. She has no impairment in her level of consciousness. She has no significant past medical history of note and is not on any chronic medications. A mini mental state examination was done for her (MMSE) and she was scored 26 out of 30. What is the most likely diagnosis for this patient?
Correct Answer : A
Signs of Alzheimer’s include:
• Memory lapses
• Forgetting the names of people and places
• Inability to remember recent events
• Problems with planning and decision-making
• Confusion
• Wandering, disorientation
Schizophrenia is characterized by false beliefs, confusion, and auditory hallucinations.
Q.18. A 50 year old diabetic woman presents with facial asymmetry to the GP surgery. The right hand corner of her mouth started drooping this morning with dribbling. She had pain behind her right ear yesterday but without any obvious rashes seen. She also complains of dryness in her right eye. On examination, she is unable to move her right side of her face or raise her right eyebrow. What is the most likely diagnosis?

Correct Answer : C
Bell’s palsy is the most likely diagnosis here although it is very important in clinical practice to exclude the remaining disorders. Bell’s palsy may present with pain around the ear during the early days.
Ramsay-Hunt syndrome may present similarly to this but usually with an association with an ear rash.
Antivirals would be appropriate for such a presentation.
Parotid tumours can also compress the facial nerve causing facial palsy however this stem did not include any mass or swelling around the jaw.
Multiple sclerosis is an upper motor neuron disease which would mean that she would be able to raise her eyebrow.
Treatment of Bell's Palsy :
- Within 72 hours on set, give prednisolone (also in pregnancy)
- Acyclovir if suspecting
Which side of the face is affected by Bell’s palsy?
Answer: The patient’s right face (i.e. right facial nerve) is affected. He is trying to smile and only his left facial muscles are working.
Q.19. A 51 year old man presents with worsening difficulty in swallowing and progressive weakness in his limbs. He is known to have motor neuron disease which has been progressively worsening over the years and is now bedridden. Hiswife, who has accompanied him says that he is unable to perform everyday tasks with one hand and that he is unable to eat properly of which he sometimes chokes when eating. On examination, he is noted to have a significant slur and is seen drooling. What is the best method to provide nutrition in this patient?
Correct Answer : C
When people with amyotrophic lateral sclerosis can no longer get enough nourishment from eating, it is advisable to insert a feeding tube into the stomach. This method is called percutaneous endoscopic gastrostomy. Since this patient is having difficulty eating and since this is a chronic degenerative condition in which long-term feeding is required, this is the single best method to provide adequate nutrition to him.
The use of a feeding tube also reduces the risk of choking and aspiration pneumonia. The tube is not painful and does not prevent people from eating food orally if they wish.
Dietitians advise preparing numerous small meals throughout the day that provide enough calories, fiber, and fluid for patients with ALS.
Q.20. A 33 year old woman previously in good health presents with sudden onset of severe occipital headache and vomiting a few hours ago. Her only physical sign on examination is a stiff neck. What is the most likely diagnosis?
Correct Answer : B
Sudden onset severe occipital headache and vomiting with stiffness make the likely diagnosis to be subarachnoid haemorrhage. The neck stiffness is due to meningeal irritation. Usually, patients would be complaining of photophobia as well. Patients often describe the headaches as “the worst headache of my life”.
Q.21. A 65 year old woman with difficulty in swallowing presents with an aspiration pneumonia. She has a bovine cough. Her tongue looks wasted and sits in the mouth with fasciculations. It is very difficult for her to articulate certain words. Sometimes as she swallows food, it comes back through her nose. What is the most likely cause of her dysphagia?
Correct Answer : D
Given her symptoms of dysphagia, tongue fasciculations, nasal regurgitations, and dysarthria, the likely diagnosis is bulbar palsy.
The phrase "A bovine cough" is used to describe the non-explosive cough of someone unable to close their glottis. It is seen in vagus nerve lesions and may be associated with dysphonia.
Bulbar relates to the medulla. Bulbar palsy is the result of diseases affecting the lower cranial nerves (VII-XII).
Presentation :
• Tongue - weak and wasted and sits in the mouth with fasciculations.
• Drooling - as saliva collects in the mouth and the patient is unable to swallow (dysphagia).
• Dysphonia - a rasping tone due to vocal cord paralysis; a nasal tone if bilateral palatal paralysis.
• Articulation - difficulty pronouncing “r”; unable to pronounce consonants as dysarthria progresses.
Q.22. A 22 year old female was hit on her side of her head with a cricket ball during a match. She initially lost consciousness but spontaneously recovered but is now experiencing increasing headache with one episode of vomiting. Her roommate has noticed that there is a slowing of responses. What is the most likely diagnosis?
Correct Answer : C
The case stem for epidural haemorrhage usually has a young athletic patient that had a head injury during a sports match. They will experience a “lucid interval” before having a decrease in mental function. The stem may or may not give you a CT brain result: “bi-convex” mass.
Q.23. A 49 year old man first presented with increasing difficulty in swallowing. Several months later he developed weakness in his right foot. Now he can no longer feed himself, he chokes on food and has become confined to a wheelchair. What is most likely diagnosis?
Correct Answer : D
This picture is of amyotrophic lateral sclerosis with bulbar onset. In MND, motor nerves become damaged and eventually stop working.
Therefore, the muscles that the damaged nerves supply gradually lose their strength.
The main types of MND are:
Amyotrophic lateral sclerosis (ALS) : This is the classical MND and the most common type. Symptoms tend to start in the hands and feet. The muscles tend to become stiff as well as weak at first.
Progressive bulbar palsy (PBP) : The muscles first affected are those used for talking, chewing, and swallowing (the bulbar muscles). This is an uncommon form of MND. The small muscles of the hands and feet are usually first affected but the muscles are not stiff.
Primary lateral sclerosis (PLS) : This is a rare type of MND. It mainly causes weakness in the leg muscles. Some people with this type may also develop clumsiness in their hands or develop speech problems.
The only subtype that has the potential to be asked is Amyotrophic lateral sclerosis (ALS)
Q.24. A 63 year old man presents after having a seizure. He is alert and oriented. On examination, in attention on the left side is noticed with hyperreflexia of the arm. What is the most likely diagnosis?
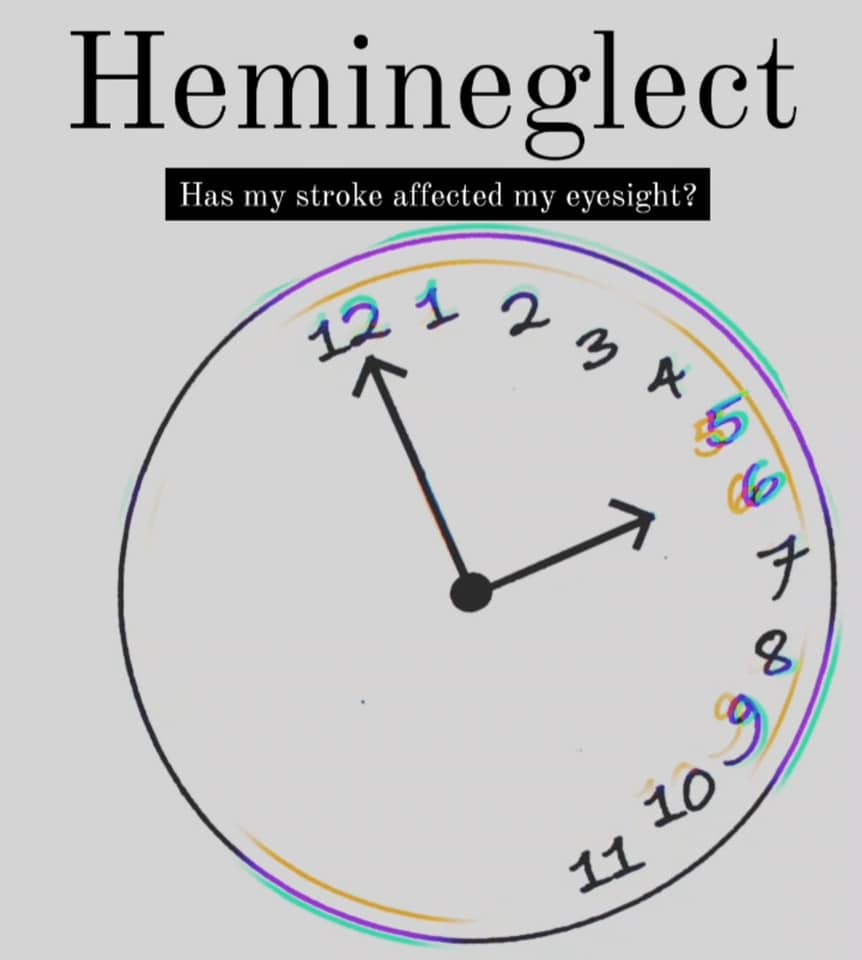
Correct Answer : C
Inattention or neglect is a feature of parietal lobe lesions. Seizures may occur in space-occupying lesions.
The most likely explanation for this answer is that the cerebral tumour has caused the right parietal lobe of the brain to be affected which can lead to neglect for the left side of the visual field, causing a patient with neglect to behave as if the left side of sensory space is nonexistent (although they can still turn left).
Q.25. A 62 year old man presents with his daughter to the clinic with complaints of visual hallucinations and features of cognitive impairment including memory loss. His symptoms of attention and levels of consciousness seem to fluctuate. He has a tremor and a festinating gait. What is the most likely diagnosis?
Correct Answer : A
The most important features of Lewy body dementia that differentiate it from the other forms of dementia are the:
• Visual hallucinations
• Fluctuating course with lucid intervals
• Signs of mild Parkinsonism
Two of which are found in this stem: signs of parkinsonism and visual hallucinations.
Q.26. A 75 year old lady on warfarin for atrial fibrillation is brought into clinic by her daughter. Her daughter is concerned as her mother is progressively getting more confused over the last couple of weeks. On physical examination, the lady was noticed to have bruises on her arms. She has an INR of 7. What is the most likely diagnosis?
Correct Answer : D
She is an elderly lady on anticoagulation. A trivial fall may have gone unnoticed. Warfarin and a high INR are risk factors for a subdural haemorrhage. Progressive confusion over days to weeks supports this diagnosis.
Q.27. A 56 year old male has increased thirst and increased micturition. He drinks around 6 litres of fluids a day. He is a known liver cancer patient and is suspected to have brain metastasis. He is awaiting an MRI of his head. Where is the most likely location for the tumour?
Correct Answer : C
This is most likely a diagnosis of Diabetes Insipidus.
The diencephalon consists of the thalamus, the hypothalamus, the epithalamus, and the subthalamus. The most likely location for an intracranial tumour causing diabetes insipidus would be the diencephalon.
In contrast, the most likely location for a brain tumour causing SIADH (Syndrome of Inappropriate Antidiuretic Hormone) would be the cerebrum or cerebellum. Both DI and SIADH are common in cancer patients or those with brain tumours so it is important to know the most likely tumour locations causing these diseases.
DIABETES INSIPIDUS TYPE AND FEATURES :
Cranial DI :
• Decreased secretion of ADH reduces the ability to concentrate urine and so causes polyuria and polydipsia.
Nephrogenic DI :
• Decreased ability to concentrate urine because of resistance to ADH in the kidney.
Q.28. A 33 year old patient presents with gradual onset of headache, neck stiffness, photophobia and fluctuating loss of consciousness. Cerebral spinal fluid shows lymphocytosis and decreased glucose but no organism on Gram stain. A CT head was read as normal. What is the most likely causative organism?
Correct Answer : B
Tuberculous meningitis would show lymphocytosis and decreased glucose.
Characteristic CSF findings in meningitis:
Bacterial meningitis:
Glucose- Low Protein, High White cells - mainly neutrophils
Viral meningitis:
Glucose-Normal, Protein-Normal to high, White cells-Increased lymphocytes
Tuberculous meningitis:
Glucose- low Protein, high White cells-Neutrophils in early disease, lymphocytes later
Q.29. A 67 year old main with a known case of diabetes mellitus type II and prostate carcinoma presents to clinic with back pain, groin numbness, and inability to initiate vomiting. Which of the following is the most likely mechanism to explain for these symptoms?
Correct Answer : B
The questions are usually very straightforward. They would usually only ask for diagnosis, investigation, and management. However occasionally, there would be a few odd questions where they would ask for the mechanism behind certain pathology.
In this case stem, the patient has a history of prostate carcinoma; therefore, the symptoms presented here would most likely indicate metastasis/tumour that is compressing on the cauda equina.
Option A would produce a degree of voiding dysfunction but not in the initiation of voiding and there would not be sensory changes.
Option C although possible will not produce severe back pain or perineal numbness.
Cauda Equina syndrome :
- Severe back pain - “saddle distribution sensory loss”
- Difficulty to initiate voiding
- Urinary or faecal incontinence
- Distal motor weakness
Diagnosis:
- MRI spine
Treatment:
- This is a neurosurgical emergency and needs a neurosurgery referral.
Q.30. A 42 year old woman has been treated with breast-conserving therapy plus systemic chemotherapy for breast cancer 6 months ago. She presents to Accidents & Emergency with a gradually worsening headache over the past week associated with nausea and vomiting and was admitted under the medical team. She has a normal neurological exam with a Glasgow Coma scale of 15. Her pulse rate is 88 beats/minute and her blood pressure is 140/80 mmHg. A non-contrast CT of the head shows a large intra-axial space occupying lesion with surrounding oedema and mass effect. What is the most appropriate next step in management?
Correct Answer : A
The imaging features are consistent with cerebral metastases which likely originated from the breast by haematogenous spread. The key treatment components of patients with cerebral metastasis revolve around the control of peritumoral oedema and control of high intracranial pressure of which corticosteroids do the trick.
Q.31. The daughter of a 69 year old male found her father alone in his apartment with confusion, bruising on his left arm and an unsteady gait. CT brain reveals a midline shift away from the side of a clot. What is the most likely diagnosis?
Correct Answer : C
In most subdural haemorrhage case stems for exam, most will present as elderly and male (chronic subdural haemorrhage). Pay attention to history details such as history of falls or other trauma.
Subdural haemorrhage :
- Fluctuating levels of consciousness
- Physical or intellectual slowing
- Sleepiness, headache, personality changes
- Unsteadiness - Seizures
Diagnosis:
- CT brain / MRI brain : Clot +/- midline shift & “crescent-shaped” haematoma
Treatment: Evacuation via burr hole craniotomy.
Q.32. A 66 year old man, known case of uncontrolled hypertension, presents to the clinic with his wife complaining of deterioration of his memory and confusion. He has a past history of transient ischaemic attack where he temporarily suffered from left arm paralysis. Throughout the year, his wife has noticed a decline in his memory, along with clumsy gait which has made him prone to falls, as well as proressive incontinence. He is a heavy smoker. On examination, his BMI is 31 kg/m2 and has an irritable mood. He scores 19 out of 30 on his mini-mental status examination. An MRI of the brain was requested and showed multiple subcortical lacunar old infarcts. What is the most likely diagnosis?
Correct Answer : B
The exam clues for vascular dementia: > 50 years with a history of smoking, hypertension, and past stroke or transient ischaemic attack.
Cardiovascular risk factors would ALWAYS be present in the stem. Often there would be a “step-wise” deterioration of symptoms.
Q.33. A 54 year old man had a recent stroke. He now presents with ataxia, intentional tremors and dysarthria. Which part of the brain is most likely affected by the stroke?
Correct Answer : C
The ataxia, intentional tremors, and dysarthria point towards a cerebellar disorder.
Aetiology includes stroke or transient ischaemic attack (TIA)
Presentation : As the cerebellum is associated with motor control, lesions produce a range of movement disorders (ataxias). Lesions of the midline vermis of the cerebellum cause truncal ataxia, while lesions of the cerebellar hemispheres cause limb ataxia of the ipsilateral side.
Q.34. A 55 year old male has a history of slurred speech and left arm weakness that lasted for 5 minutes and resolved completely. An ECG performed in the Emergency Department showed a heart rate of 80 beats/minute in sinus rhythm. He takes regular antihypertensive medications. He does not have any other medical conditions. He was discharged from the hospital and asked to be seen in a TIA clinic for follow up. What is the most appropriate long term medication(s) to be prescribed.
Correct Answer : D
Post-management of Transient ischaemic attack (TIA) Clopidogrel (75 mg daily) is the preferred long-term antiplatelet (off-label use in TIA). Current guidelines recommend treatment with high-intensity statin following a TIA for all patients unless contraindicated.
Q.35. A 70 year old man with a known case of ischaemic heart disease presents to emergency with paralysis of his left arm, sensory loss on the left side of his face, right sided gaze preference and homonymous hemianopsia. Which of the following is the most likely artery to be affected?
Correct Answer : B
For exam, stroke questions come in various forms ranging from the anatomical locations of the lesion, to investigations and management. Pay special attention to the anatomy of the lesions especially the vascular distribution and the functions of the different parts of the brain. i.e. anterior cerebral artery
– frontal and medial cerebrum : middle cerebral artery
– lateral part of the hemisphere : posterior cerebral artery
– occipital lobe : basilar artery
Q.36. A 64 year old man presents to the Accident & Emergency department with a history of left sided hemiparesis and slurred speech that started earlier today. His symptoms resolved and he was completely asymptomatic 6 hours after the episode. A CT scan of his head revealed no acute haemorrhage. What is the most appropriate prophylactic regimen?
Correct Answer : D
Post-management of Transient Ischaemic Attack (TIA) : Aspirin is given for 2 weeks followed by clopidogrel (75 mg daily) as clopidogrel is the preferred long-term antiplatelet for secondary prevention.
If clopidogrel is contraindicated or not tolerated, give a combination of modified-release dipyridamole (200 mg twice daily) and low-dose aspirin. A statin should also be offered as soon as possible after a TIA.
Q.37. A 24 year old woman complains of progressive left leg stiffness and clumsiness over the past few weeks. There has also been a history of intermittent blurry vision that spontaneously resolves each time. On examination, there is increased tone, left leg power of 3/5, and upward plantars. A pale disc was seen on ophthalmoscopy. All other neurological examinations were normal. What is the most appropriate initial management?
Correct Answer : A
This patient is presenting with upper motor neuron signs and optic neuritis. The diagnosis is relapsing-remitting multiple sclerosis. The patient is eligible for interferon-beta management; however, the question asks for the most appropriate initial management, which in this case would be methylprednisolone.
Q.38. A 72 year old man with a history of hypertension and an ex-smoker presents to the clinic with his wife due to change in behaviour. For the past year and a half, he has slowly become socially withdrawn with a decreased interest in his usual hobbies. There are times where he forgets to groom himself and there was an incident once where his wife found him urinating on the sofa. Over the past few months there has been a gradual struggle with finding the right word choice while talking. What is the most likely diagnosis?
Correct Answer : B
The keys, in this case, stem: the patient has been struggling with word choice (temporal lobe) and disinhibition / urinating on the sofa (frontal lobe).
Alzheimer’s disease usually presents with memory loss first before personality changes.
Vascular dementia would have a “step-wise progression” and they would have had some sort of previous cardiac/vascular event in the stem.
Lewy body disease would require a clue into having some Parkinsonian symptoms.
Q.39. A 50 year old man complains of being pursued by the police for a crime he denies committing however on further investigation, this was found to be untrue. He has poor concentration and impaired short-term memory. He admits to drinking large amounts of alcohol for the last 20 years. He is able to carry on a coherent conversation, but moments later he is unable to recall that the conversation took place. What is the most likely diagnosis?
Correct Answer : C
This is termed Wernicke-Korsakoff syndrome and is characterized by the addition of Antero- and retrograde amnesia and confabulation in addition to the classic triad of confusion, ataxia, and ophthalmoplegia found in Wernicke's encephalopathy.
Those with Korsakoff syndrome may "confabulate," or make up, information they can not remember. They are not "lying" but may believe their invented explanations. They create events to fill the gaps in day-to-day memory.
For example, a person who has been in hospital for several weeks may talk convincingly about having just visited their aunt earlier that day. This is more common in the early stages of the condition. Individuals may seem able to carry on a coherent conversation, but moments later be unable to recall that the conversation took place or to whom they spoke.
They can often answer questions promptly with inaccurate and sometimes bizarre answers.
Q.40. A 79 year old stumbled at home and sustained a minor head injury 2 weeks ago. He did not become unconscious and was well after the fall. His son has brought him to clinic because he has become increasingly confused, drowsy and unsteady over the past few days. He has a GCS of 13. His past medical history includes atrial fibrillation which he takes warfarin for. What is the most likely diagnosis?
Correct Answer : D
An elderly man with a history of falls and on anticoagulation with progressive confusion over the last couple of days points towards the diagnosis of chronic subdural haemorrhage. Chronic subdural haematoma occurs in very old or severe alcoholics.
A shrunken brain is rattled around the head by minor trauma, tearing venous sinuses. Over several days or weeks, mental function deteriorates as haematoma forms.
CT scan is diagnostic, and surgical evacuation provides a dramatic cure. Remember, Chronic subdural haematoma usually presents as an elderly, on anticoag or an alcoholic who may have a history of falls. Slow onset of symptoms compared to epidural haematoma.
Q.41. A 53 year old man presents to clinic with complaints of urinary incontinence and erectile dysfunction. He is seen to have ataxia, rigidity and a pill rolling tremor of the hands. On examination, postural hypotension is also noted. What is the most likely diagnosis?
Correct Answer : A
Shy-drager syndrome : A rare neurodegenerative disorder, caused by cell loss in certain areas of the brain and the spinal cord, leading to a variety of symptoms characterized by Parkinsonian features, cerebellar ataxia, and autonomic dysfunction (particularly urogenital).
Presentation:
• Urinary dysfunction is the most common presentation
• Erectile dysfunction
• Postural hypotension
• Cerebellar ataxia
• Parkinsonian symptoms with poor response to levodopa.
In the exam, if you get a stem with characteristics of parkinsonism (rigidity, pill-rolling tremor of the hands) plus autonomic dysfunction like urinary incontinence, erectile dysfunction, consider Shy-drager syndrome as the answer.
Q.42. An 8 year old girl is brought to the clinic due to abnormal behaviour noticed by her teacher. She would stare blankly towards the wall, sometimes with an upturning of the eyes for around 15 seconds, then blinks. This would occur several times during the day. The teacher notes that while she would resume her activity after these events she would be tired and unable to concentrate. What is the most likely diagnosis?
Correct Answer : B
Absence seizures would usually be a child with either the parent or teacher noticing that the patient is “daydreaming” often and when they resume their studies they are not able to perform well.
Absence seizure :
- Child usually <10 years old
- Loss of awareness (“daydreaming”), staring blankly into space, will not respond to their surroundings
- May be accompanied by upturning of eyes, other repetitive movements
- Will return to normal activities after a seizure but may not perform well and feel tired
- No photosensitivity
- Maybe triggered by hyperventilation
Diagnosis:
- EEG
- Check FBC, glucose levels, ECG, and MRI for other underlying causes
Treatment: - If recurring, sodium valproate or ethosuximide.
Q.43. A 34 year old housemaid presents with severe headaches in the back of her head for several days and pain on flexing her neck. The pain is worsened by movements. On examination, there is limited range of movement of the neck. What is the most likely diagnosis?
Correct Answer : A
Cervical spondylosis is chronic cervical disc degeneration with herniation of disc material, calcification, and osteophytic outgrowths.
Headache in the back of the head and pain in flexing the neck is an early feature of cervical spondylosis which gradually progresses to later symptoms like radiculopathies due to root compression in arms and hands.
Q.44. A 33 year old man presents with speech difficulties. He has an irregular breakdown of articulation. On examination, nystagmus is seen. Which anatomical site is most likely to be affected?
Correct Answer : B
It is quite unclear what sort of speech difficulties this patient has. However with a combination with nystagmus, one can assume that this patient is having cerebellar dysarthria (also known as ataxic dysarthria).
Cerebellar dysarthria is an acquired neurological and sensorimotor speech deficit caused by damage to the superior cerebellum and the superior cerebellar peduncle.
If, for example, there is damage to the left cerebellar hemisphere in a right-handed person, ataxic dysarthria could develop. Of all the individual dysarthria types, it most clearly reflects a breakdown in timing and coordination.
Q.45. A 32 year old female presents with a history of recurring headaches. They are usually unilateral, last for 24-48 hours, have a pulsatile quality, and are associated with nausea and photophobia. The patient describes the headaches as intense, usually requiring her to limit her activities. She has tried several over-the-conter medications with no relief. Which of the following is the most appropriate choice for first-line management of her condition?
Correct Answer : C
This is a classic presentation of acute migraine. First-line therapy is triptans according to NICE guidelines.
Be aware that opioids are never given during an acute onset of migraine.
Migraine :
• History of unilateral, throbbing headache
• Associated with nausea / vomiting, photophobia
• Associated with aura/triggers
• May be described as: “need to limit activities” or “prefer to stay in a dark room”
Diagnosis:
• Clinical diagnosis
• May require CT / MRI head to rule out other pathology
Treatment:
• Sumatriptan - first line
• Monotherapy: Triptan, NSAIDs, Aspirin, Paracetamol
• Combination therapy: Triptan + NSAID; Triptan + Paracetamol
• Transcutaneous stimulation of the vagus nerve
• Avoid triggers.
Q.46. A 68 year old lady complains of falls to the ground without any warning. She maintains consciousness throughout and remembers the event. There is no confusion after the fall. What is the most likely diagnosis?
Correct Answer : D
Drop attacks are sudden spontaneous falls while standing or walking, with complete recovery in seconds or minutes. There is usually no loss of consciousness, and the event is remembered.
The remaining options given usually have a prodrome or identifiable symptoms before the episodes like dizziness or pallor.
Drop attacks refer to unexplained falls with no prodrome, no loss of consciousness, and rapid recovery.
The proportion of falls due to ‘drop attack’ increases with age.
Causes :
• Vertebrobasilar insufficiency
• Weak legs (eg cauda equina syndrome)
Note that the usual cause is sudden weakness of the legs that causes the patient, usually an older woman, to fall to the ground.
There is no warning, no loss of consciousness, and no confusion afterward.
The condition is usually benign, resolving spontaneously after several attacks.
Q.47. A 50 year old man presents to the clinic with his wife. She states that her husband has had a noticeable change in personality. He is impulsive and occasionally demonstrates inappropriate behaviour. On examination, he has difficulty naming objects, but his memory, ability to calculate, and his visuospatial skills are intact. What is the most likely diagnosis?
Correct Answer : C
The hallmark of Pick’s disease is behavioral changes, inappropriate behavior, and disinhibition. In the early stages of Pick’s disease memory, visuospatial skills, and calculation are relatively intact and this differs from Alzheimer’s where usually memory would be affected first.
Q.48. A 58 year old woman presents with acute onset of back pain following a rough and long journey in a car. On examination, there is tenderness at the mid-thoracic vertebra. The pain goes away when she bends forward. What is the most likely diagnosis?
Correct Answer : A
Myofascial pain syndrome is a chronic pain disorder characterized by regional muscle pain associated with restricted painful regions or trigger points. The pain is often aching and deep in nature. Myofascial pain syndrome typically occurs after a muscle has been contracted repetitively.
In this case, the long car ride journey has caused muscles to contract repetitively. In the options given, only myofascial pain/muscle sprain relieves on change of position.
The trapezius, levator scapula, infraspinatus, and scales are commonly affected areas but in this question with the mid-thoracic vertebra, it is likely the trapezius that is affected the most. The remaining options are wrong.
Osteoporotic fracture of the vertebrae would cause severe pain which will not improve on bending or any movement.
Q.49. A 26 year old woman who is a known epileptic wants to start a family. She takes sodium valproate for her epilepsy which has been well controlled and has been seizure free for the past year. She and her husband have been using condoms as contraception till present. She attends clinic seeking advice regarding her antiepileptic medication as she would like to get pregnant. What is the most appropriate advice to give?
Correct Answer : B
Change to carbamazepine is the best option given the options provided. If there was an option that said, to change to carbamazepine and add folic acid 5mg, that would be an even better answer. One would not stop antiepileptic medication especially if the patient has only been seizure-free for one year.
The patient needs to be seizure-free for more than 2 years before it would be considered reasonable to stop antiepileptic medication before pregnancy.
If a woman is taking antiepileptic drugs and planning a pregnancy, the general advice to give to her is about the increased risks of fetal malformations, neurodevelopmental delay, and possible increased seizure frequency in pregnancy. Since there is no agreement as to which antiepileptic drug is most or least teratogenic, the antiepileptic drug that stops seizures in a given patient is the one that should be used.
However, there is one exception to the rule, SODIUM VALPROATE! The risk of teratogenicity with Valproate is greater than the risk of teratogenicity with other antiepileptic drugs. Hence, sodium valproate should always be changed to another antiepileptic drug before pregnancy.
Q.50. A 44 year old lady with established multiple sclerosis attends A&E with the complaint of weakness and a reduction in sensation on the left side of her face. She also complains of hearing loss in her left ear, as well as unsteadiness when she tries to walk. She is noted to have difficulty in coordinating her hand movements. What is the most likely neuroanatomical structure affected?
Correct Answer : A
The lesions of multiple sclerosis most commonly affect the white matter in the optic nerve, brainstem, basal ganglia, and spinal cord, or white matter tracts close to the lateral ventricles.
The brainstem provides the main motor and sensory innervation to the face and neck via the cranial nerves.
It includes the midbrain, the medulla oblongata, and the pons. Since this patient is experiencing deficits in her trigeminal nerve (CN V) and her vestibulocochlear nerve (CN VIII), this answer makes the most sense.
Q.51. A 73 year old male presents with a history of falls over the past 12 months. His relatives have also noticed a rather strange behaviour lately and more recently he has had episodes of enuresis. Examination reveals that he is disoriented to time and place with a broad-based, clumsy gait. What is the most likely diagnosis?
Correct Answer : B
The history of falls and broad-based clumsy gait (balance and gait disturbance), strange behavior and disorientation to time and place (due to dementia), and episodes of enuresis (urinary incontinence) point towards normal pressure hydrocephalus.
Normal pressure hydrocephalus will present with prominent gait abnormalities early in the course of the disease that usually precede the onset of cognitive impairment. There will also be associated urinary incontinence. Normal pressure hydrocephalus is a reversible cause of dementia seen in elderly patients.
It is thought to be secondary to reduced CSF absorption at the arachnoid villi. Has a classical triad of:
• Urinary incontinence
• Dementia
• Gait abnormality (may be similar to Parkinson's disease)
“the wet, wobbly and wacky grandpa”
Q.52. A 49 year old chronic alcoholic with established liver damage is brought to the hospital after an episode of heavy drinking. He is not able to walk straight and is complaining of double vision. He is shouting obscenities and expletives. What is the most likely diagnosis?
Correct Answer : C
Wernicke's encephalopathy is a neuropsychiatric disorder caused by thiamine deficiency which is most commonly seen in alcoholics. A classic triad of confusion, ophthalmoplegia, and ataxia may occur.
Treatment is with urgent replacement of thiamine (vitamin B1).
If not treated Korsakoff's syndrome may develop as well. This is termed Wernicke-Korsakoff syndrome and is characterized by the addition of Antero- and retrograde amnesia and confabulation in addition to the above classic triad.
Q.53. A 2 year old child is brought to the Paediatric Accidents & Emergency by his parents as they are worried about the possibility of their son having a seizure. Earlier today he fell from his bicycle but made no sound then becomes pale. This was accompanied by a stiffening, clonic jerks of the limbs and loss of consciousness. He regains full consciousness a few seconds later. What is the most likely diagnosis?
Correct Answer : B
When a toddler cries after a minor injury, stops breathing, and loses consciousness for a few seconds followed by rapid recovery, you should be thinking of two conditions:
1. Blue breath-holding spells
2. Reflex anoxic seizures are paroxysmal, spontaneously reversing brief episodes of asystole triggered by pain, fear, or anxiety. They are non-epileptic events caused by a reflex asystole due to increased vagal responsiveness.
They begin when a toddler typically aged from 6 months to 2 years has a sudden surprising pain or an unexpected fright, stops breathing then goes pale, rigid, and may have upward eye deviation with clonic movements.
These episodes last less than a minute and it is followed by rapid recovery. Management is just reassurance and advises parents to place the child in a recovery position during episodes.
Remember: Reflex anoxic seizures do not cause tongue biting – An important point when differentiating from epilepsy.
Q.54. A 44 year old woman presents with a severe throbbing unilateral right sided headache and photophobia 20 minutes after an episode of tingling and numbness of her left hand. What is the most likely diagnosis?
Correct Answer : D
This is a typical case stem for migraine in exam. The patient will present with or without aura (sensory or motor) followed by the headache itself.
THIS IS EXTREMELY IMPORTANT.
The key to differentiating between a migraine or a headache of a more serious origin (e.g. subarachnoid hemorrhage) is the onset of a unilateral, throbbing headache AFTER an aura.
Q.55. A 72 year old woman is seen to collapse by her son. He calls the paramedics when she is unable to stand and seems weak down her right side. On arrival to the A&E her GCS is 13/15 with a right hemiparesis. She is increasingly agitated and within an hour her GCS is 8/15. Which is the most appropriate next course of action?
Correct Answer : A
Anaesthetic review would be the next most appropriate step of action. The history and examination are convincing for a stroke but the patient has rapidly dropped her consciousness levels, and before any investigations and treatment can happen this needs to be addressed.
An anaesthetist would rather know at this stage rather than when a peri-arrest call is put out as her GCS reaches 4 or 5. The airway can be stabilized so that a CT scan can be performed safely.
The other options are less likely to be the appropriate next course of action. Thrombolysis or aspirin are the treatment options for ischaemic strokes but cannot be started until a CT scan excludes a haemorrhage.
Q.56. A 32 year old female who is 18 weeks pregnant presents to the Emergency Department. She has a history of epilepsy and is on medication for it however she was non-compliant and did not take her medication for the past 5 days. She had a tonic-clonic seizure earlier in the morning lasting for 5 minutes and was brought in by ambulance. She has IV access. While waiting for a doctor, she starts to have another generalized tonic-clonic seizure. What is the most appropriate management?
Correct Answer : B
Seizures lasting longer than 5 minutes should be treated urgently with intravenous lorazepam (repeated once after 10 minutes if seizures recur or fail to respond).
Intravenous diazepam is effective but it carries a high risk of thrombophlebitis (reduced by using an emulsion formulation). Absorption of diazepam from suppositories is far too slow for the treatment of status epilepticus.
The fact that she is pregnant does not change the management of a convulsive status epilepticus.
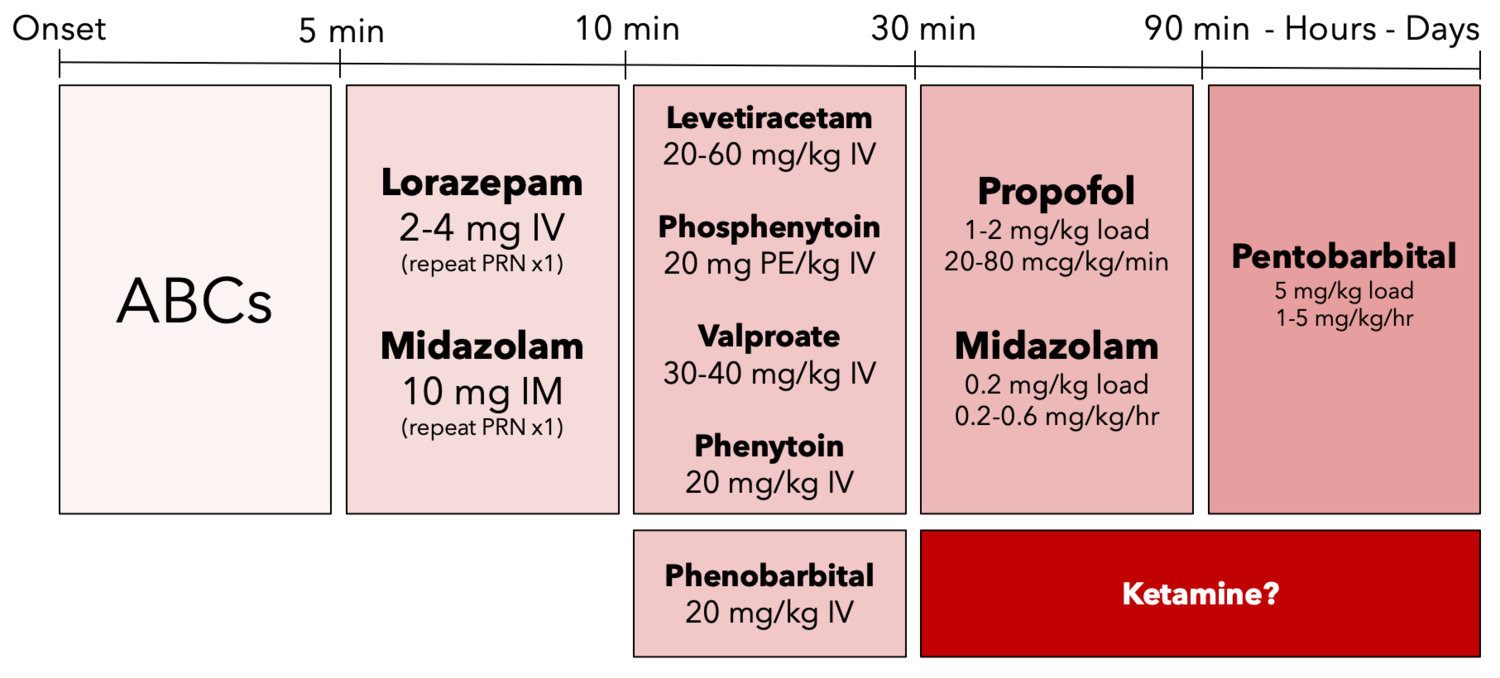
STATUS EPILEPTICUS MANAGEMENT:
• ABC protocol
• Give high-concentration oxygen
• Check blood glucose levels
• Secure intravenous access in a large vein
• Administer intravenous lorazepam as first-line treatment in hospital for ongoing generalised tonic-clonic seizures
• Administer intravenous diazepam if intravenous lorazepam is unavailable, or buccalmidazolam if unable to secure immediate intravenous access. Administer a maximumof two doses of the first-line treatment (including pre-hospital treatment)
• If seizures continue, administer intravenous phenobarbital or phenytoin as a second-line treatment in hospital
• If seizure continues despite the above (>30 minutes), referral to ICU.
Q.57. A 39 year old chronic alcoholic stopped drinking alcohol for the last 2 days. He presents to A&E with symptoms of feeling anxious, having tremors and is seen sweating profusely. His heart rate is 103 beats/minnute. What is the most appropriate treatment?
Correct Answer : A
The patient presents with symptoms of acute alcohol withdrawal. This patient would require benzodiazepines as part of his management and would need to be referred to the medical team from A&E. IV Thiamine would also be given in the hospital. This is to help prevent Wernicke’s encephalopathy.
Q.58. A 71 year old lady has a history of a fall 3 days ago with an injury to the head. She is increasingly drowsy and has recently become confused and disoriented. What is the most likely vessel to be involved?
Correct Answer : D
The clinical symptoms match those of a chronic subdural haematoma. This would be caused by a rupture of a bridging vein. Among the options given, the cerebral vein would be the most likely. Chronic subdural haematoma occurs in very old or severe alcoholics.
A shrunken brain is rattled around the head by minor trauma, tearing venous sinuses. Over several days or weeks, mental function deteriorates as haematoma forms. CT scan is diagnostic, and surgical evacuation provides a dramatic cure.
Q.59. A 40 year old man who has recently lost his job was found to be stumbling and wandering around the local partk, muttering to himself with plans to kill himself. The police have brought him to the hospital in an unkempt and disheveled state and he displays a general level of bad hygiene. He is pale and smells of stale sweat. The police officer who brought him to the hospital says that he had administered an alcohol breath test for the patient which showed zero percent of alcohol. In addition, the patient appears to be confused and is unable to answer most of your questions. What is the best initial management for this patient?
Correct Answer : D
This is a classic case of alcohol withdrawal, which develops about 12 to 24 hours after the drinking abruptly stops. The symptoms can last for days afterward. The fact that the stem gives you that this patient has lost his job, is unkept and smells of stale sweat sounds much like there is a background of alcoholism in this picture.
Benzodiazepines would be the most appropriate initial management as they help with alcohol detoxification.
Q.60. A 35 year old lady is seen by a Neurologist for funny turns. These episodes were witnessed by her husband who describes15 minute episode of inability to talk without losing consciousness. This has been ongoing every 2-3 days since the sudden unexpected death of her mother 2 months ago. What is the most useful investigation to help aid in diagnosis?
Correct Answer : C
Video electroencephalogram : This investigation will help rule out any form of epilepsy.
Q.61. A 42 year old female had a sudden onset of severe headache and vomiting. She took paracetamol and an hour later she collapsed. Her medical history is significant for Ehlers-Danlos syndrome. What is the most likely diagnosis?
Correct Answer : A
Sudden onset of severe headache, vomiting then collapse are more suggestive of subarachnoid haemorrhage.
This is also supported by the medical history of Ehlers-Danlos syndrome.
Occasionally the stem would include signs of meningeal irritation. This includes neck stiffness and photophobia. Patients often describe the headaches as “the worst headache of my life”.
Q.62. A 67 year old woman with a history of atrial fibrillation presents to emergency with slurred speech, asymmetric facial weakness, left sided hemiparesis and ataxia. On arrival to the A&E, her GCS is 14/15. She is increasingly agitated. Which is the most appropriate next course of action?
Correct Answer : B
The history and examination are convincing for a stroke. Before any treatment can happen we need to exclude a haemorrhagic stroke with the help of imaging. This was done in this question which showed an ischaemic stroke. The next step is to start thrombolytics.
The other options are less likely to be the appropriate next course of action.
Anticoagulants should not be started until brain imaging has excluded haemorrhage, and usually not until 14 days have passed from the onset of an ischaemic stroke.
Thrombolysis or aspirin are the treatment options for ischaemic strokes but cannot be started until a CT scan excludes a haemorrhage.
Q.63. A 35 year old woman complains of dizziness. She awoke in the morning with a mild headache and dizziness started when she sat up in the bed. She felt that the room was spinning for a few minutes. If she is at rest the spinning stops but is aggravated by movement. There are no other neurological symptoms. What is the most likely diagnosis?
Correct Answer : D
All of the above options are popular topics in exam.
Meniere’s disease usually involves tinnitus, deafness, and increased ear pressure in the case stem.
Vestibular neuronitis, while similar to Meniere’s does not have hearing loss.
Acoustic neuroma as it grows into the cerebellopontine angle would involve cranial nerves V, VII, and VIII; therefore, you would have a variation of symptoms involving these three nerves.
Between options A and B, the symptoms in the case stem would not spontaneously resolve for option A.
Q.64. A 62 year old male is brought to the emergency department by his daughter as he is confused, and has an unsteady, uncoordinated walking. He is a known alcoholic and has been admitted recently with delirium tremens. On questioning, he denies any problem with his memory. He knows his name and address and convincingly states that he was at a betting shop in the morning. His daughter interjects saying that, that is untrue as he was at home. What is the most likely diagnosis?
Correct Answer : C
Please see Q-39
Q.65. A 78 year old woman admitted for a urinary tract infection for the last 10 days has become increasingly confused. Her son has noted her level of consciousness has been fluctuating and is disoriented to time and place. She is more withdrawn but intermittently becomes very noisy and agitated. What is the most likely diagnosis?
Correct Answer : B
For the exam, it is important to know the difference between dementia and delirium.
The onset of delirium is more acute with fluctuating levels of consciousness. There will be disorientation, mood changes, paranoia, and some memory impairment. Urinary tract infections are a common cause of delirium in the elderly.
Delirium Presentation:
• Acute onset
• Fluctuating levels of consciousness
• Often in the elderly
• Disorientation, mood changes, paranoia
• Memory impairment
• Abnormalities of perception e.g. hallucinations or illusions
• Withdrawn or heightened arousal
Common precipitating factors
• Metabolic derangement
• Hypoxia
• Infection
• Dehydration
• Constipation
• Medications e.g. benzodiazepines
Treatment:
• Treat underlying cause
• Consider anti-psychotics.
Q.66. A 78 year old male presents with a history of urinary incontinence and change in behaviour. On examination, he has a waddling gait. What is the most likely diagnosis?
Correct Answer : A
Please see Q-13
Q.67. A 79 year old man was seen in the memory clinic as an outpatient. On his mental state examination, he was noted to be disengaged, expressing boredome as well as making inappropriate comments to the doctor of a sexual nature. What is the most likely diagnosis?
Correct Answer : C
The patient in this scenario is exhibiting signs of disinhibition. This feature is most characteristically seen in those with frontotemporal dementia. They may also have features of insisting on ingesting sweet things as well as angry and violent outbursts.
Alzheimer’s disease is not correct as in Alzheimer’s disease, patients classically show signs of reduced function such as the reduced ability to speak with eventual aphasia.
To help remember, think of the three A’s: apraxia (inability to carry out purposeful movements), aphasia (loss of ability to speak), and agnosia (loss of ability to recognize what objects are and do as well as people).
Huntington’s disease is not correct as this is primarily a neurological disorder that is characterized by movement
Lewy Body dementia is not correct as the characteristic features here include increased risk of falls as well as visual hallucinations.
Cerebrovascular accident is not the correct answer as this is more typically characterized by motor/sensory loss of function.
Q.68. A 44 year old woman has a two week history of electric shock-like stabbing facial pain starting from her left jaw and radiates towards her forehead. The pain is unilateral and it is descrbed as very severe and coming in spasms. The pain is trigerred by chewing but occurs at other times as well. Her corneal reflexes are found to be normal. What is the most likely diagnosis?
Correct Answer : D
Electric shock-like, sharp, shooting, and stabbing are features usually used to describe trigeminal neuralgia.
Trigeminal neuralgia :
• Unilateral, shooting, or stabbing electric shock-like facial pain
• Pain exacerbated with movement or touch especially in the jaw (CN V, 2nd and 3rd branch distribution)
• Abrupt in onset and termination
Diagnosis :
• Clinical
• MRI is routinely done to rule out other pathology (i.e. schwannoma, meningioma)
Treatment :
• Medication then surgery
• Carbamazepine > Lamotrigine / phenytoin / gabapentin
• Surgical: Microvascular decompression
The corneal reflex in this stem is intact which makes the the choice of answer clearer.
Q.69. An 80 year old man has had an ischaemic stroke and was brought to the A&E department 6 hours after the onset of symptoms by his concerned daughter who found him lying on the floor at home. A CT brain has already been done and has confirmed the diagnosis. The patient has no drug allergies and no other comorbidities. What is the most appropriate medication to be given to this patient upon discharge?
Correct Answer : C
Post management of Transient ischaemic attack (TIA), Stroke :
Clopidogrel (75 mg daily) is the preferred long-term antiplatelet. If clopidogrel is contraindicated or not tolerated, give a combination of modified-release dipyridamole twice daily and low-dose aspirin.
Ensure a statin has been offered as soon as possible after a TIA Stroke.
Aspirin 300 mg daily for 2 weeks is given immediately after an ischaemic stroke is confirmed by brain imaging.
Q.70. An 8 year old boy developed a seizure first affecting his right arm. The seizure lasted for several minutes. He was unconscious throughout the seizure and has no recollection of the events that occurred leading to his seizure. A computed tomography scan of his head was organized after the seizure and has been reported as having a lesion on the left cerebral hemisphere. What is the most likely reason for his seizure?
Correct Answer : D
This boy has just had a complex partial seizure. The term “partial” (or focal) seizure means that the electrical activity is limited to a part of one cerebral hemisphere. The term “complex” seizure means there was the loss of awareness. The seizure is likely caused by the lesion seen on the CT scan that is occupying space.
Epilepsy - is incorrect as the termed epilepsy would require at least two unprovoked seizures occurring more than 24 hours apart for the definition to fall into place.
Dementia - is incorrect as dementia is a brain disorder causing memory loss and decline in cognition. It occurs in the elderly and does not cause seizures.
Huntington’s chorea - is also incorrect. Firstly, symptoms of Huntington’s disease become noticeable between the ages of 35 and 44 years old. This boy is too young to develop symptoms of Huntington’s disease. Secondly, Huntington’s chorea is characterized by jerky, random, and uncontrolled movements.
Q.71. A 5 year old girl is brought to the hospital by her mother with complaints of sudden right facial weakness, numbness and pain around her ear. She reports no other symptoms. On examination, her right eyebrow is unable to raise and the right hand corner of her mouth is drooping. What is the most likely diagnosis?
Correct Answer : D
These are classic features of Bell’s palsy. Bell’s palsy can strike anyone at any age although less common than 15.
Facial weakness presentations at a young age like this stem usually warrant an urgent referral to pediatrics as Bell’s palsy is less likely to be a cause and should be investigated for other potential reasons. This question however clearly points towards the diagnosis of Bell’s palsy.
Q.72. A 33 year old man was working late in his office when he had a sudden onset of an excruciating headache localized to his right side and associated with right eye pain. He has had similar episodes 2 months ago. On examination, his right eye is swollen and red with lacrimation. What is the most likely diagnosis?
Correct Answer : B
For the exam, it is important to know how to differentiate the different types of headaches (e.g. intracerebral haemorrhage, migraine, cluster headache, tension headache)
Features of a cluster headache in the exam usually include a male undergoing some sort of activity with a rapid onset of a severe headache with eye involvement.
The eye pain is usually periorbital. As the name implies, the frequency of these headaches occurs in “clusters”.
Look at the time frame in the stem: there is usually a clue to having frequent past episodes with/without a period of remission.
CLUSTER HEADACHE :
- Excruciating headache: Pain is often worse compared to tension-type headaches or even migraines.
- Unilateral orbital, supraorbital, temporal - Intermittent for days to years
- Pain description can vary (can be sharp, burning, or throbbing)
- Triggers include stress, alcohol, exercise
- Accompanied by redness, lacrimation, lid swelling, nasal stuffiness
- Intense pain around one eye (recurrent attacks 'always' affect the same side). Pain is so severe that patients are often restless or agitated.
Management:
- Acute: sumatriptan subcutaneous + 100% oxygen
- Prophylaxis: Calcium channel blockers (verapamil)
Q.73. A 64 year old housewife, who is a known case of uncontrolled hypertension, presents to Accident & Emergency with the complaints of dysphagia, right sided hemiparesis and ataxia. She also reports a loss of sensation on the right side of her face and a loss of sensation on her left leg. Which of the following is the most likely area in the brain to be affected?
Correct Answer : C
Stroke questions come in various forms ranging from the anatomical locations of the lesion, to investigations and management. Pay special attention to the anatomy of the lesions especially the vascular distribution and the functions of the different parts of the brain. In this case stem, the vascular system affected is the vertebrobasilar circulation.
Therefore, symptoms will arise from one or all of the following areas: cerebellum, brainstem, and occipital lobes.
Q.74. A 65 year old man has been recently diagnosed with atrial fibrillation. He has suffered from a transient ischaemic attack 3 years ago. His medical history is significant for diabetes mellitus type 2. What is the best scoring method to assess for anticoagulation?
Correct Answer : D
Knowing the contents of the ABCD2 and the CHA2DS2-VASc scoring system is necessary for the exam and knowing when to apply each scoring system is vital.
The ABCD2 score is to assess the risk of future stroke in the next 7 days in patients who have already suffered from a transient ischaemic attack (TIA).
After a TIA, early recurrent stroke is common. Around 10-15% have a second TIA/CVA in the first week often within the first 48 hours. The ABCD2 score helps the physician decide on how to manage the patient.
The CHA2DS2-VASc score is to assess the risk of future stroke in patients who have atrial fibrillation. This score is then used to determine whether or not treatment is required with anticoagulation therapy.
Remember:
ABCD2 = Risk of future stroke following TIA because of how soon to refer to a specialist.
CHA2DS2-VASc = Risk of future stroke in patients with atrial fibrillation because of the necessity of anticoagulation therapy (Warfarin or Aspirin)
Q.75. A 50 year old lady presents with a sudden onset of severe occipital headache associated with neck pain and vomiting. CT brain was inconclusive and a lumbar puncture was performed which revealed xanthochromia. What is the best likely diagnosis?
Correct Answer : A
The case stems from subarachnoid haemorrhage usually middle-aged patients with sudden, severe onset headaches, which may be described as “the worst headache of their lives” or “thunderclap headache”. This is also important to note since there are middle cerebral artery [MCA] occlusions (due to ischaemia) and
MCA berry aneurysms (causing subarachnoid haemorrhage). Ischaemic occlusions would usually have more stroke symptoms provided in the stem such as motor and sensory loss, rarely presenting with headache.
Q.76. A 52 year old woman diagnosed with breast cancer presents with urinary frequency and extreme thirst. She finds herself passing large amounts of urine even at night. Which part of the brain is the metastasis likely to have spread to?
Correct Answer : C
The topic to be discussed here is Diabetes Insipidus which accounts for her urinary frequency. In this question, cranial diabetes insipidus is described. It is due to a deficiency of circulating arginine vasopressin (antidiuretic hormone). The pathophysiology behind this is pituitary infiltration by metastases originating from the breast.
A little anatomy knowledge is needed in this question. Among all of the answers, the diencephalon would fit as it gives rise to the posterior forebrain structures including the thalamus, hypothalamus, posterior portion of the pituitary gland, and pineal gland.
Q.77. A 45 year old man has back pain radiating down to his legs. He has motor weakness with knee extension and foot dorsiflexion. On examination, perineal sensory loss is noted. What is the most appropriate action?
Correct Answer : D
This is a classic example of cauda equina syndrome. It is a serious neurologic condition in which damage to the cauda equina causes loss of function of the nerve roots of the spinal canal below the termination (conus medullaris) of the spinal cord.
Any lesion which compresses or disturbs the function of the cauda equina may disable the nerves although the most common is a central disc prolapse. Spinal cord compression or cauda equina syndrome are neurological emergencies that require immediate referral and intervention.
The management of true cauda equina syndrome frequently involves surgical decompression. Pain due to a herniated lumbosacral disc may settle within six weeks. If it does not, or there are red flag signs such as the possibility of cauda equina syndrome like in this case, referral to an orthopaedic surgeon or a neurosurgeon should be considered.
Red flags that suggest cauda equina syndrome include:
• Severe or progressive bilateral neurological deficit of the legs, such as major motor weakness with knee extension, ankle eversion, or foot dorsiflexion
• Recent-onset urinary retention or urinary incontinence
• Recent-onset faecal incontinence
• Saddle anaesthesia or paraesthesia
Q.78. A 55 year old was admitted to the hospital for investigations of haemoptysis. Two days after admission he develops alternating state of consciousness, sweating, and tremors. His temperature is 37.3 C. He gives a history of drinking alcohol every day for the past year. What is the most appropriate management?
Correct Answer : A
These are features of acute alcohol withdrawal. Chlordiazepoxide would help reduce his symptoms.
Q.79. A 28 year old attends the GP surgery wanting advice on combined oral contraceptive pills. She has been taking combined hormonal contraception for the past year but has recently developed symptoms of migraines. She read online that combined hormonal contraception should not be used in migraine with aura sufferers. Which of the following is a characteristic of a migraine with aura?
Correct Answer : C
The reason combined hormonal contraception is not used in patients with migraine with aura is that they have a 2-4 time added risk of cerebrovascular accident. It is quite important to remember the differences between migraines with and without auras.
Auras can be described as warning signs before the headache begins.
Aura characteristics:
• Occurs before the onset of headache
• Lasts 5 to 60 minutes
• Visual symptoms (homonymous hemianopia, fortified spectra, scotoma), unilateral paraesthesia or weakness, dysphasia.
• Headache either begins before the end of the aura or within an hour of the end
Migraine with aura is an absolute contraindication to using the combined oral contraceptive pill due to an increased risk of cerebrovascular accidents. Mirena IUD is adviced in patients who suffer from migraine with aura.
Q.80. A 43 year old chronic alcoholic stopped drinking alcohol for the last 3 days. He is anxious, has tremors and is now having hallucinations. His heart rate is 106 beats/minute. What is the most appropriate treatment?
Correct Answer : A
Benzodiazepines are the recommended drugs for alcohol detoxification. They have a slower onset of action and therefore are less likely to lead to abuse. A reduced dose of chlordiazepoxide is commonly used. Diazepam is an alternative. In this particular case, he has hallucinations which are a sign that he is having not just an acute alcohol withdrawal but moving on to delirium tremens.
Patients with marked agitation or hallucinations and those at risk of delirium tremens (characterized by delirium, hallucinations, coarse tremor, and disorientation) may be prescribed antipsychotic drugs, such as haloperidol or olanzapine, as adjunctive therapy to benzodiazepines.
Q.81. A 75 year old woman has been admitted from a nursing home with sudden onset of right hemiplegia and homonymous hemianopia. She is dysphasic. She remains conscious throughout and on examination, brisk reflexes and several beats of clonus are noted. What is the most likely artery to be occluded?
Correct Answer : B
This patient has an upper motor neuron lesion as signified by a pathological extensor plantar response and hyperreflexia. Every option that was given could cause the symptoms of stroke. However, it is important to know which is the most common artery to be occluded in stroke. This would be the middle cerebral arteries.
Q.82. A 54 year old patient is seen at the clinic for muscle weakness. His muscle weakness initially started at the level of his legs but now it is affecting his arms too. On examination, he has loss of tendon reflexes and decreased muscle strength. What is the most likely mechanism of this weakness?
Correct Answer : C
You should suspect Guillain-Barre syndrome in ascending symptoms of paresthesia in line with the recent gastroenteritis. The pathophysiology is complicated but you would need to remember that it is an acute inflammatory demyelinating neuropathy.
GUILLAIN-BARRÉ SYNDROME :
Guillain-Barre syndrome Is a disorder causing demyelination characterized by weakness, paresthesia, and hyporeflexia. Around two-thirds precedes an infection, usually the respiratory or gastrointestinal tract.
This association with the preceding infection suggests that antibodies to the infectious organism also attack antigens in peripheral nerve tissue. In the stem, there would usually be a history of gastrointestinal or respiratory infection from anywhere between a few days to 3 weeks before the onset of weakness.
Presentation:
• Weakness - Presents with an ascending pattern of progressive symmetrical weakness, starting in the lower extremities. Reaches a level of maximum severity two weeks after the initial onset of symptoms. Facial weakness, dysphasia, or dysarthria. In severe cases, muscle weakness may lead to respiratory failure.
• Pain - Neuropathic pain, particularly in the legs
• Reflexes - Reduced or absent
• Sensory - Paresthesia and sensory loss, starting in the lower extremities.
Q.83. A 45 year old man with terminal cancer who has recently completed his course of chemotherapy develops tingling and numbness of the fingertips of both arms. He describes a constant mild burning discomfort in his hands and feet. Occasionally, he experiences a sharp, shooting, and electric-shock like pain in his feet. What is the most likely cause of his symptoms?
Correct Answer : D
Chemotherapy drugs such as vincristine are known for the side effects of peripheral neuropathy due to neurotoxicity.
Patients with this side effect would present with peripheral paraesthesia which is seen as numbness or tingling. Chemotherapy-induced peripheral neuropathy is typically characterized by a glove-and-stocking distribution in the hands and feet with sensory loss or hypersensitivity and in some cases motor and autonomic dysfunction.
Q.84. A 52 year old lady has weak limbs when examined. She was found to have burn marks on fingertips. Her hands looked wasted and with diminished reflexes. She also has weak spastic legs and dissociated sensory loss. What is the most likely diagnosis?
Correct Answer : A
If you were to see burn marks on your fingertips in any given question, think of a loss of sensation of temperature and pain in the hands. This is commonly seen in syringomyelia and syringobulbia. The wasted and weak hands with diminished reflexes and weak spastic legs with dissociated sensory loss are features suggestive of syringomyelia.
Syringomyelia and Syringobulbia : Syringomyelia is a rare condition in which there is a fluid-filled tubular cyst (syrinx) within the central, usually cervical, spinal cord. This leads to various neurological symptoms and signs, including pain, paralysis, stiffness, and weakness in the back, shoulders, and extremities.
Syringomyelia may also cause loss of extreme temperature sensation, particularly in the hands, and a cape-like loss of pain and temperature sensation along the back and arms. Syringobulbia occurs when the syrinx extends into the brainstem. This may affect one or more cranial nerves, resulting in facial palsies. Sensory and motor nerve pathways may be affected by interruption and/or compression of nerves
. Note: Progression of symptoms and deterioration occur over many years for syringomyelia and syringobulbia Symptoms of both Syringomyelia and Syringobulbia
• Damage to the spinal cord often leads to progressive weakness in the arms and legs, stiffness in the back, shoulders, arms, or legs, and chronic, severe pain. These can be presented at the presentation.
• Other symptoms may include headaches, a loss of the ability to feel extremes of hot or cold (especially in the hands), and loss of bladder and other functions.
• Pain and temperature sensation are lost due to spinothalamic tract damage
. • Classically, the sensation loss is experienced in a shawl-like distribution over the arms, shoulders, and upper body.
• Dysaesthesia (pain experienced when the skin is touched) is common.
• Light touch, vibration, and position senses in the feet are affected as the syrinx enlarges into the dorsal columns.
• Muscle wasting and weakness begin in the hands and then affect the forearms and shoulders.
• Tendon reflexes are lost.
Q.85. A 26 year old female presents with bladder incontinence, clumsiness when walking, shooting lower back pain, and blurry vision, and sensory loss. These symptoms have occurred all at once or in different combinations approximately every few months and each event lasts 3-4 days. There is swelling of the optic disc on fundoscopy, inability to walk heel to toe, and weakness at the hip girdles. What is the most appropriate diagnostic test?
Correct Answer : D
This is a diagnosis of multiple sclerosis. The definitive diagnostic test would be an MRI brain and spinal cord.
This patient is presenting with upper motor neuron signs and optic neuritis. Multiple Sclerosis Presentation: A variety of symptoms involve motor and sensory mainly of the brainstem and cerebellum. It may be easier to divide them into groups to remember.
1. Transverse myelitis:
• Weakness, sensory symptoms
• Urinary urgency and retention
• Flexor spasms
• Spastic quadriparesis or paraparesis
• 2. Brainstem:
• Ataxia
• Diplopia
• Dysarthria
• Facial numbness
• Ophthalmoplegia
• Gaze palsy
• 3. Cerebellum
• Ataxia • Dysarthria
• Nystagmus
Question usually has some clue to optic neuritis. Optic neuritis is an acute, sometimes painful, reduction or loss of vision in one eye and is a relatively common presenting symptom of MS. Colour vision may be impaired
• Also depression is common The pattern is usually: symptoms evolve over days, plateau, then resolve over days/weeks
Diagnosis:
• Mostly a clinical diagnosis
• MRI (definitive diagnostic test): demyelination and/or lesions disseminated in time and place
• Oligoclonal bands in CSF
Treatment:
• Acute: IV or oral methylprednisolone
• Interferon-beta or glatiramer acetate (first line).
Q.86. A 30 year old primigravida woman of 32 weeks gestation presents to clinic with left facial droop of 2 days duration. On examination, there is no rash. The nasolabial fold is flattened, there is a drooping of the left corner of her mouth when asked to smile, and eye closure is weaker on the left side. She is unable to puff her cheeks or wrinkle her forehead. What is the most likely cause to these clinical findings?
Correct Answer : D
Cranial nerve palsies for CN III, VI, and VII are very commonly asked. In addition to the clinical findings on examination, another exam clue pointing to this diagnosis is the “pregnancy in the third trimester”. Bell’s palsy is three times more common in pregnancy. Another scenario that may be given would be a patient who is diabetic.
Look closely at the age: If the examiners would want you to pick stroke, they would have given a much older patient and they would provide some findings of upper/lower limb deficit.
There is no travel history or going to the jungle; therefore, this option is unlikely. Option B would have a prior infection in the case stem and would most likely present with a rash. Bell’s palsy is a diagnosis of exclusion.
So be sure to exclude all other possibilities in practice before you label someone with Bell’s palsy. One special take-home point is that if the patient can close their eyes and raise their eyebrow on the affected side, then it is NOT Bell’s palsy, but an upper motor neuron lesion. Bell’s palsy is a lower motor neuron facial nerve palsy.
Q.87. A 38 year old heroin addict was involved in a car crash and, as a result, is now paraplegic. He was agitated and cried every day during the first two weeks after accident while he was in the hospital. Upon questioning, he was unable to remember the accident at all and refused to talk about it. What is the most likely diagnosis?
Correct Answer : A
The likely diagnosis here is organic brain damage as he is unable to remember the accident. One can easily exclude post-traumatic stress disorder with that history as patients with PTSD are quite the opposite and would remember the experience and have flashbacks and nightmares about it. It is normal to have an amount of sadness after a major accident that involves brain injury.
This differs from severe depression, as symptoms of severe depression interfere with normal function. If the severity of sadness persisted and there was a degree of functional impairment and disability associated with low mood, then we would be able to say that this is severe depression. Symptoms of an organic brain injury may include confusion, impairment of memory, and agitation which can be seen in this stem.
Q.88. A 22 year old female presents with progressive difficulty in walking due to lower back pain. There is tingling and numbness in her hands that has radiated towards her elbows. On examinatioin, cranial nerves are intact. There is no sensation of vibration or pin prick in her upper limbs to elbows and from lower limbs to hips. There are absent reflexes and mute plantars. Blood pressure is 124/85 mmHg and heart rate is 68 beats/minute. The patient had an episode of food poisoning two months ago. What is the most likely diagnosis?
Correct Answer : D
Key features for case stem: young female with ascending polyneuropathy usually after a trigger (i.e. infection).
There are absent reflexes therefore multiple sclerosis is ruled out since it involves upper motor neurons. Myasthenia gravis usually would have more emphasis on fatigue especially in the proximal muscles and cranial nerves would be affected.
There is no clue in the stem that the patient is diabetic and even if he is, the onset is acute while option D would require a more gradual progressive process.
While the patient did have an infection, there was no history of travel and for option E to occur it would most likely be a diagnosis of Lyme disease.
Q.89. A 55 year olf chronic alcoholic who lives alone, brought in the emergency department having been found confused at home after a fall. He complains of a headache and gradually worsening confusion. What is the most likely diagnosis?
Correct Answer : C
A chronic alcoholic with a history of falls with progressive confusion over the last couple of days points towards the diagnosis of chronic subdural haemorrhage. Subdural haematoma may be acute or chronic. In chronic subdural haematoma, symptoms may not be apparent for several days or weeks.
Symptoms of subdural haematomas are: fluctuating level of consciousness, ± insidious physical or intellectual slowing, sleepiness, headache, personality change, and unsteadiness.
A chronic subdural haematoma occurs in very old or severe alcoholics. A shrunken brain is rattled around the head by minor trauma, tearing venous sinuses. Over several days or weeks, mental function deteriorates as haematoma forms. CT scan is diagnostic, and surgical evacuation provides a dramatic cure.
Remember, chronic subdural haematoma usually presents as an elderly, on anticoagulation, or an alcoholic who may have a history of falls. Slow onset of symptoms compared to epidural haematoma.
Q.90. An 18 year old female presents to the Emergency Department with a generalized tonic-clonic seizure. Her seizure had lasted 20 minutes according to eyewitness accounts. Her SpO2 is currently 97% and she has already been given 2 doses of rectal diazepam but the seizures have not stopped. What is the most appropriate management?
Correct Answer : C
The diagnosis here is status epilepticus. The patient continues to have a seizure despite 2 doses of diazepam. Therefore, the next appropriate management would be phenytoin infusion. If the patient was not given two doses of rectal diazepam in the community, then we would administer IV lorazepam as first-line treatment in the hospital. However, because two doses of diazepam were given (most likely in the community), we would move to second-line which would be IV phenytoin.
Preference goes to IV phenytoin before using IV phenobarbital.
If this also fails then the next step would be referral to ICU and then consider intubation. For exam, know the initial management of all acute neurological emergencies.
Note that buccal midazolam is usually the first-line treatment in children, young people, and adults with prolonged or repeated seizures in the community. However, if buccal midazolam is unavailable, rectal diazepam is used. Hence, the probable reason why rectal diazepam was used in this stem.
Note that the management for ongoing generalized tonic-clonic seizures (convulsive status epilepticus) in the hospital is different from the community. Below we will only discuss management in the hospital.
Q.91. A 34 year old man is hit by a car. He loses consciousness but is found to be fine by the paramedics. When awaiting doctor’s review in the Emergency Department he suddenly becomes unconscious. What is the most likely diagnosis?
Correct Answer : D
This patient has lucid intervals. It is important to note that acute subdural haematoma also has lucid intervals. And thus when a patient presents with lucid intervals it can be both an extradural haematoma or an acute subdural haematoma. In general, for extradural haematoma the trauma is usually trivial and the patient goes back to doing what he was doing before falling unconscious again.
Whereas acute subdural haematoma is usually a sicker patient who barely awakes during lucid intervals.
But again in clinical practice, we do not lie on clinical features to differentiate epidural haematoma from acute subdural haematoma because both of them will get a CT scan Also, note the difference between acute subdural haematoma and chronic subdural haematoma.
In chronic subdural haematoma, it is usually elderly, on anticoag, or an alcoholic. Symptoms for chronic subdural haematoma are slow onset compared to epidural haematoma. As this question did not specify whether subdural haematoma is acute or chronic, it would be more correct to choose extradural (epidural) haematoma as the answer.
Extradural (epidural) haematoma Often associated with skull fracture and middle meningeal artery injury. Involves arterial blood.
Features :
• Features of raised intracranial pressure
• Patients may exhibit a lucid interval.
Management :
Surgical procedure: burr hole over pterion (to ensure that further haemorrhage escapes instead of expanding the clot further) followed by craniotomy and evacuation of the haematoma.
Q.92. A 31 year old man, known case of alcohol abuse, is brought into Emergency by his friend from a nightclub. The friend saw the patient suddenly collapse on the dance floor where his body went stiff then there was twitching of his legs followed by involuntary voiding. When he gained consciousness, he was drowsy and confused for several minutes before full recovery. What is the most likely diagnosis?
Correct Answer : B
Know the difference between generalized and partial seizures. Generalized seizures usually have patients with a loss of consciousness (i.e. “collapsed”) while partial seizures may or may not have a loss of consciousness depending if they are simple or complex. When both halves of the body (right and left) are involved, it is classified as generalized.
In this case, this patient’s seizure activity is due to alcohol abuse and therefore should follow guidelines on management related to seizures secondary to alcoholism.
Stiffness is the tonic phase followed by twitching which is the clonic phase. Myoclonic seizures are irregular jerks of the trunk or limbs that occur while the patient is conscious and last for less than a second.
Most of us have this experience when we are falling asleep and suddenly jerk as if we fell from a building. That is considered a normal phenomenon. Myoclonic seizures in an awake state are not normal and require specialist assessment.
Q.93. A 33 year old woman has pain and a funny sensation in her legs especially at night when she sleeps. Her symptoms have been ongoing for the past 3 months. She describes the funny sensations as having insects crawling up her legs which wake her up at night. She finds relief almost immediately when she moves her legs. She has no previous psychiatry history of note. Her blood results show: Haemoglobin 140 g/L Ferritin 250 ng/ml. Which of the following medications is effective in treating this condition?
Correct Answer : A
Restless legs (previously called Willis-Ekbom syndrome) are common and can be very disturbing. The typical features include the urge to move (usually legs). It is often accompanied by the abnormal sensation of aching or tingling and in some, pain is a feature.
The symptoms tend to appear in the evening. They are also more commonly seen in pregnant women and often worsen as pregnancy progresses. The symptoms are relieved by moving. Useful advice includes avoiding alcohol, smoking, and caffeine.
Exercise and good sleep hygiene have been shown to benefit symptoms. It is common to measure serum ferritin levels in people suffering from restless legs syndrome as restless legs syndrome is associated with iron deficiency hence the reason the values were given in this stem. If ferritin is low, start iron supplementation, despite normal haemoglobin levels.
Since in this question, ferritin levels are within normal limits, she would not require iron supplementation. Only around 20% of sufferers would need a drug treatment.
Common medications used for the treatment of restless leg syndrome include:
• Dopamine agonist
• Gabapentin
• Pregabalin
Q.94. A 50 year old woman presents following a fall. She reports pain and weakness in her hands for several months, swallowing difficulties, and has bilateral wasting of the small muscles of her hands. Her back and shoulders feel stiff. The reflexes in her upper limbs are absent. Both legs show increased tone and hyperreflexia. Pain and temperature sensation are impaired in the upper limbs. She is also noted to have a facial palsy. What is the most likely diagnosis?
Correct Answer : B
There are two close answers here: syringobulbia and syringomyelia. Syringomyelia does not have any cranial nerve involvement but syringobulbia does and thus causing the facial palsy in the above question.
Q.95. A 53 year old chronic alcoholic was brought to the emergency department with an alternating state of consciousness, nausea and vomiting. He has unsteady, uncoordinated walking and complains of double vision. On examination of his face, his eyelids seem to be drooping and nystagmus is seen. He denies having taken alcohol in the last 12 hours. What is the most appropriate management?
Correct Answer : B
This man is suffering from Wernicke’s encephalopathy. Eye-movement abnormalities seen in Wernicke’s encephalopathy include gaze-evoked nystagmus, spontaneous upbeat nystagmus, and horizontal or vertical ophthalmoplegia. Wernicke's encephalopathy is a neuropsychiatric disorder caused by thiamine deficiency which is most commonly seen in alcoholics.
A classic triad of confusion, ophthalmoplegia, and ataxia may occur. Treatment is with urgent replacement of thiamine If not treated Korsakoff's syndrome may develop as well.
This is termed Wernicke-Korsakoff syndrome and is characterized by the addition of Antero- and retrograde amnesia and confabulation in addition to the above classic triad.
Q.96. A 31 year old woman, no known cae of medical illnesses, presents to clinic with numbness and tingling of her hands and fingers followed by a severe throbbing headache localized to her left side. At home she tried to relieve her headache with cold packs, paracetamol, and ibuprofen but there was no relief. She has had similar episodes in the past. Currently, she is nauseated. On examination, she required the lights to be dimmed. What is the most appropriate next step pharmacological management?
Correct Answer : D
This is a typical case stem for migraine. The patient will present with or without aura (sensory or motor) followed by the headache itself. To differentiate from more serious headaches (i.e. intracranial haemorrhages), the clues usually would be “throbbing headache”, unilateral, and/or photophobia.
Note that topiramate is teratogenic/causes embryopathy and is a preventative measure for migraine. Also, pay attention to what question asks: If the woman is on COCP and has migraine with aura, advise cessation of COCP as it increases the risk of ischemic stroke.
Q.97. A 7 year old child is brought to the hospital by his teacher. The child was playing with other children and suddenly fell down and hit the table and went unconscious for a few seconds before returning to his normal self. On probing further, the diagnosis of absence seizure was made. What is the most likely reason that could have led to this diagnosis?
Correct Answer : C
Absence seizures would usually be a child (<10 years) with either the parent or teacher noticing that the patient is “daydreaming” often and when they resume their studies they are not able to perform well.
In this scenario, however, the diagnosis was already given but they want you to know what is the history that could give you the diagnosis. Staring blankly into space upturning of eyes for a few seconds and resuming activity almost immediately is indicative of absence seizures.
Q.98. A 31 year old man with no past medical history complains of severe headache since 2 hours ago during work. The headache is mainly localized to the left side and is associated with photophobia. A similar episode had occurred a few months ago which also involved his left side. It had lasted for several minutes for several times a day for a period of 2 weeks and resolved spontaneously. During this examination, he is unable to sit still with obvious agitation and anxiety. What is the most likely diagnosis?
Correct Answer : A
For exam, make sure you can differentiate the different types of headaches (tension, cluster, migraine). Cluster headache case stems usually have a young male with a headache localized to one side along with some autonomic features. Also, there should be a history of episodes over a couple of weeks. Another clue is people with cluster headaches usually move around while in migraines they tend to be lying down in a dark room.
Q.99. A previously healthy 20 year old woman presents to the Emergency Department with the complaint of “falling out”. She was with her friends at a restaurant when she felt faint and, according to friends, lost consciousnes for about a minute. There was no seizure activity noted, but the friends did notice her arms twitching irregularly. She is now acting normally. She denies chest pain or palpitation, and her electrocardiogram is normal. What is the most likely diagnosis?
Correct Answer : C
Have a basic idea of the major causes of syncope. The most common amongst young women would be vasovagal syncope likely due to hypotension and stimulated by one of the following triggers: pain, fear, excitement, and standing for a prolonged period. Vasovagal syncope
Presentation:
• Young adults more common than women
• Stimulated by either emotional stress or orthostatic stress
• Sweating, pallor, nausea Diagnosis:
• Clinical history under recommended diagnostic criteria (ESC guidelines)
• ECG to rule out other pathology
Treatment:
• Reassurance and counseling of avoidance of triggers
• Educate how to recognize prodromal symptoms and perform manoeuvres to stop the syncope
• Tilt table training
Q.100. A young man who has just moved to new accommodation presents with severe lower back pain lasting for 2 weeks. It is worse at the end of the day. His gait is normal. There are no red flag symptoms or signs. He is otherwise well. What advice would you give him?
Correct Answer : D
This man is suffering from mechanical lower back pain. He should continue to mobilize and take regular analgesia (not just when required).
Of note, he may have been doing some heavy lifting while moving to his new accommodation which has exacerbated the condition. He does not have any red flags.
Red flags for lower back pain are :
• Age over 50 years or under 18 years old
• Unexplained weight loss > 10 kg within 6 months
• Night pain or pain at rest
• Pain persists for more than 6 weeks
• Failure to improve with therapy
• History of cancer
• Urinary incontinence or retention
• Faecal incontinence
• Saddle anaesthesia
• Progressive neurological deficit
• Vertebral tenderness
Bed rest is not recommended. The current guidance is to continue mobilizing and consider an exercise program. Spinal manipulation therapies can be offered as part of a treatment package including exercise.
NICE guidelines on lower back pain do not recommend acupuncture for lower back pain. Paracetamol alone is not effective for the treatment of lower back pain.
Q.101. A 40 year old woman with a history of epilepsy presents to the clinic with multiple fleshy nodules and several light brown, round macules with a smooth border on her back, arms and legs. There are also freckles under her arms. What is the most likely diagnosis?
Correct Answer : A
While this is more of a dermatology / connective tissue topic than a neurology topic, neurofibromatosis type I (NF1) does present with neurological deficits.
Know how to differentiate between type I and type II as well as the basic management.
Neurofibromatosis type I :
• Cafe au lait spots, axillary freckling and neurofibromas
• Lisch nodules (hamartomas on the iris)
• Optic gliomas
• Scoliosis, bone dysplasias
• Epilepsy / seizures
• Cognitive impairment
Treatment:
• Conservative
• Routine monitoring and counselling
• Neurofibromas - if irritation, removal by laser or surgical
• Malignant peripheral nerve sheath tumors - radiation and surgical excision.
Q.102. A 49 year old patient has Parkinson’s disease. What is the most useful medication in the management of his tremor and dystonia?
Correct Answer : B
Benzhexol is an anticholinergic agent and it is the drug of choice to treat Parkinson’s disease-induced tremors. Anticholinergic agents have a limited role and should only be prescribed in young patients with severe tremors and dystonia. Orphenadrine is also another anticholinergic agent that is commonly used.
Q.103. A 66 year old female patient presents to Accident & Emergency with a 12 hour history of a severe headache with associated nausea and vomiting. She has no other complaints other than the headache which she describes as feeling like she was “kicked in the head”. She claims that the headache is felt worse at the back of her head. Morphine and metoclopramide has been given for the pain and a CT scan of the head was done which was reported as no acute abnormalities seen. What is the most appropriate next action in this patient’s management?
Correct Answer : C
We should be suspecting subarachnoid haemorrhage in these cohorts of patients who present this way. It is important to note that a diagnosis of subarachnoid haemorrhage cannot be made on clinical grounds alone. The following are investigative steps to take if you suspect someone has had a subarachnoid haemorrhage.
1. CT scan: CT scanning without contrast is the first line of investigation.
2. Lumbar puncture: If the CT scan is negative but the history is suggestive, a lumbar puncture should be undertaken.
3. MRI: Can be more sensitive than CT, but only after several days have passed. After a subarachnoid haemorrhage is confirmed, its origin needs to be determined. The choice between cerebral angiography and CT angiography to identify aneurysms.
Q.104. A 45 year old man has tremors in both his hands. The tremors are absent at rest but present when arms are held outstretched and persist on movement. Movements such as writing are affected by his tremor. The tremor is seen to be worse when he is tired or stressed. On examination, the tremor continues to be present even when patient is distracted. What is the most likely diagnosis?
Correct Answer : D
Know the difference between psychogenic tremors and essential tremors. The given stem has the clinical features of an essential tremor.
In psychogenic tremors, there is often an abrupt onset and spontaneous remission, and the characteristic of the tremor changes when the patient is distracted.
Parkinsonian tremors usually would have the classical sign of ‘pill-rolling’ in combination with rigidity and bradykinesia which is absent in this stem. Cerebellar disease could present with intentional tremors which is not seen in this stem.
Intentional tremors occur during voluntary active movements of the upper body. The tremor would worsen as goal-directed movement approaches its intended target. The stem would usually include overshooting or undershooting their target, a condition known as dysmetria.
It is a form of ataxia. For example, a patient would find difficulty due to his tremor when asked to touch his nose and then the examiner’s fingers. Essential tremor symptoms
• Distal symmetrical postural tremor of the upper limbs
• Initially transient. May progress to become persistent.
• Amplitude of tremor may depend on physiological or emotional state
• May be seen to improve following alcohol ingestion
• Not seen at rest
Management :
• Propranolol is the first line.
Q.105. A 45 year old man presents to the clinic for his routine diabetic check-up. Upon examination, the patient has a normal tone, 5/5 power, normal plantar reflexes and normal proprioception. There is a deficit in fine touch sensation on the medial side of the right lower leg. Which of the following is the most likely dermatome to be affected?
Correct Answer : B
These questions do sometimes appear on the exam and therefore would be useful to know.
Usually, it would be the major dermatomes of the upper and lower limbs In the exam, questions may appear with a diabetic neuropathy stem or a trauma with sensory loss. Alternatively, it may also appear as just a straightforward statement asking for the dermatome of a specific part of the body with no case stem.
Q.106. A 43 year old woman presented with blurred vision and intermittent clumsiness for 3 months. Reflexes are brisk in her arm and optic disc is pale. What is the most appropriate test to confirm diagnosis?
Correct Answer : A
She has features suggestive of multiple sclerosis. The investigation of choice is an MRI scan.
Multiple Sclerosis : A variety of symptoms involve motor and sensory mainly of the brainstem and cerebellum. It may be easier to divide them into groups to remember.
1. Transverse myelitis: Weakness, sensory symptoms - Urinary urgency and retention. Flexor spasms, Spastic quadriparesis or paraparesis.
2. Brainstem: Ataxia, Diplopia, Dysarthria, Facial numbness, Ophthalmoplegia, Gaze palsy.
3. Cerebellum - Ataxia, Dysarthria, Nystagmus
Optic neuritis is an acute, sometimes painful, reduction or loss of vision in one eye and is a relatively common presenting symptom of MS. Colour vision may be impaired.
• Also depression is common. The pattern is usually: symptoms evolve over days, plateau, then resolve over days / weeks.
Diagnosis:
• Mostly a clinical diagnosis
• MRI (definitive diagnostic test): Demyelination and/or lesions disseminated in time and place
• Oligoclonal bands in CSF
Treatment :
• Acute: IV or oral methylprednisolone
• Interferon-beta (first line).
Q.107. A 56 year old lady has developed severe right sided headache which worsens whenever she goes under the bright light. This has been occurring for the last 3 days. She feels nauseated, but has not vomited. She does not take any medication and has no relevant medical history. What is the most likely diagnosis?
Correct Answer : C
She is suffering from Migraine. The hints provided here are that it is a unilateral headache associated with photophobia and nausea. The other options given here are much less likely.
Subarachnoid haemorrhage - Usually presents with the worst headache ever. What we call a “thunderclap headache”.
Chronic Subdural haematoma - Questions usually give a history of an elderly, on anticoagulation, or an alcoholic.
Intracranial neoplasm - Possible but less likely compared to migraine. The history of headaches would usually be longer. It is a space-occupying lesion, so one can expect a raised intracranial pressure (ICP). Headache, which is typically worse in the mornings, nausea and vomiting, seizures, and papilloedema.
Cluster headache - Usually presents with intense pain around one eye accompanied by redness, lacrimation, lid swelling, and also nasal stuffiness.
Q.108. A 55 year old man presents to clinic for gradual weakness of his arms bilaterally over the past year. He is now unable to lift heavy loads above his head and has difficulty breathing while going up the stairs. In the past month, he has noticed hoarseness and difficulty in swallowing liquids. On examination, there was muscle atrophy and weakness in the trunk, neck and both proximal upper limbs for lower motor signs. Deep tendon reflexes in the upper and lower limbs were positive for upper motor signs with atrophy of the tongue. Hoffman’s sign was positive and autoimmune panel is normal. What is the most likely diagnosis?
Correct Answer : B
Amyotrophic lateral sclerosis (ALS) is the most common form of motor neuron disease in addition to multiple sclerosis (MS). Know the distinction between both for exam as they will commonly appear as either a question or an option.
MS usually presents in episodes intermittently and affects different anatomic locations.
Myasthenia gravis would present with weakness and fatigue along with a positive autoimmune panel.
Guillain-Barre syndrome would usually give a clue to a prior infection.
Polymyositis would affect the lower limbs first with fatigue.
Q.109. A 44 year old man with a history of chronic alcohol abuse attends A&E. He is unkempt, drowsy, walks with an ataxic gait and has poor memory. It is believed he has not eaten in forty eight hours. A decision to commence chlordiazepoxide and IV Pabrinex is made. Which vitamin, present in Pabrinex, can prevent the progression of his symptoms?
Correct Answer : C
This man is suffering from Wernicke’s encephalopathy. Vitamin B1, also called thiamine, is needed to treat Wernicke’s encephalopathy.
Wernicke's encephalopathy is a neuropsychiatric disorder caused by thiamine deficiency which is most commonly seen in alcoholics. A classic triad of confusion, ophthalmoplegia, and ataxia may occur.
Treatment is with urgent replacement of thiamine. If not treated Korsakoff's syndrome may develop as well. This is termed Wernicke-Korsakoff syndrome and is characterized by the addition of Antero- and retrograde amnesia and confabulation in addition to the above classic triad.
Q.110. A 26 year old woman is seen in neurology clinic with a history of 3 episodes of convulsions. Her husband has observed all three episodes. They last around 15 minutes and begin by her losing awareness and becoming unresponsive. This is followed by strange and repeated movements of her arms, legs and pelvis. During the episodes, her eyes are closed. There was no drooling of saliva, and no incontinence in any of the episodes. What is the most appropriate investigation?
Correct Answer : D
It is often difficult to tell the difference between an epileptic seizure and a non-epileptic attack disorder (NEAD) in clinical practice. Non-epileptic attacks may look like epileptic seizures but they are not caused by an electrical disturbance in the brain. From the history given, this sounds more like a non-epileptic attack disorder.
The key phrases here that point towards the diagnosis of NEAD are the pelvic movements, episodes where eyes are closed, no drooling of saliva which means the mouth is closed during the attacks, and lastly no incontinence.
Video electroencephalogram (EEG) is an investigation especially useful to diagnose NEAD or if the diagnosis is uncertain. This involves hooking up EEG equipment and also having a continuous video of the patient to capture the activity of the brain and physical movements and sounds during seizures.
Q.111. A 60 year old man presents to Emergency with dizziness. The onset was sudden and described as “the room spinning around”. He also is bumping into things on his right side. On examination, his blood pressure is 159/91 mmHg, heart rate is 72 bpm. He is positive for nystagmus and dysdiadochokinesia. CT brain confirms ischaemic stroke. Where is the most likely location of his stroke?
Correct Answer : B
Know that lesions to the posterior circulation would affect functions of the brainstem, cerebellum, and occipital lobe. This would be consistent with the vertigo, right hemianopia, nystagmus, and ataxia seen in this patient.
Stroke in the posterior circulation presentation :
• Dizziness / vertigo, right hemianopia, nystagmus, ataxia, dysdiadochokinesia
• Usually sudden onset with possible further progression that takes place over hours
• May have underlying ischaemic heart disease, hypertension, carotid bruits, atrial fibrillation
Diagnosis :
• Non-contrast CT brain - initial investigation
• MRI brain - more sensitivity
Treatment:
• Ischaemic stroke - Thrombolysis (alteplase) & aspirin
• Maintain oxygen saturation, glucose control, blood pressure control
• Maintain nutrition and hydration
• Early mobilization
Q.112. A 65 year old lady presents to the Accident and Emergency department with a 6 hour history of facial droop and weakness on her left side of her body. A CT scan was performed and ruled out a haemorrhagic stroke. She is allergic to Penicillin and takes Simvastatin and Amlodipine regularly. What is the most appropriate medication to be prescribed long term for this patient?
Correct Answer : C
The patient had an ischaemic stroke and the standard treatment would be Aspirin for 14 days, and then Clopidogrel long-term.
The question is asking for the long-term treatment and therefore this would be Clopidogrel.
Alteplase - for patients who are appropriate for thrombolysis therapy who present within 4.5 hours of the onset of stroke symptoms, and intracranial haemorrhage has been excluded by imaging techniques.
Aspirin is started as a standard therapy for confirmed ischaemic stroke and is continued until 2 weeks, at which time definitive long-term antithrombotic treatment should be initiated.
Aspirin is only recommended long-term for patients intolerant to clopidogrel.
Q.113. A 72 year old man becomes confused over a period of 2 weeks. He used to be active and goes for long walks. Now he stares at the wall, barely talks to anyone, and sleeps majority of the day. His daughter recalls that he fell down the stairs about a week before the mental changes began. What is the most likely diagnosis?
Correct Answer : A
An elderly man with a history of falls and on anticoagulation with progressive confusion over the last couple of days points towards the diagnosis of chronic subdural haemorrhage.
Chronic subdural haematoma occurs in very old or severe alcoholics. A shrunken brain is rattled around the head by minor trauma, tearing venous sinuses. Over several days or weeks, mental function deteriorates as haematoma forms.
CT scan is diagnostic, and surgical evacuation provides a dramatic cure.
Remember, Chronic subdural haematoma usually presents as an elderly, on anticoag or an alcoholic who may have a history of falls. Slow onset of symptoms compared to epidural haematoma.
Q.114. An 82 year old lady had an ischaemic stroke that was confirmed with brain imaging. She has no drug allergies and no other combordities. She was put on aspirin 300 mg daily for two weeks. What is the most appropriate medication to be given after the course of Aspirin is completed?
Correct Answer : B
Clopidogrel is now recommended by NICE ahead of the combination use of aspirin plus dipyridamole in people who have had an ischaemic stroke.
Q.115. A 69 year old woman is brought to A&E by ambulance with no significant past medical history of allergies. She presents with speech disturbance and asymmetric facial and arm weakness. The symptoms began 3 hours ago. Brain imaging shows an ischaemic stroke. What is the most appropriate next course of action?
Correct Answer : D
The history and examination are convincing for a stroke. Before any treatment can happen we need to exclude a haemorrhagic stroke with the help of imaging. This was done in this question which showed an ischaemic stroke. The next step is to start thrombolytics.
The other options are less likely to be the appropriate next course of action.
Anticoagulation should not be started until brain imaging has excluded haemorrhage, and usually not until 14 days have passed from the onset of an ischaemic stroke.
It is recommended to prefer alteplase over streptokinase.
Q.116. A 74 year old woman was brought to clinic by her daughter for confusion and memory impairment. The patient would periodically start a task and forget to finish them and has difficulty naming objects. In the past few months, she has lost 5 kg and does not sleep well at night. On examination, the patient was agitated and had decreased skin turgor, and not oriented to time or place. She repeatedly asks the same questions during the interview. What is the most likely diagnosis?
Correct Answer : A
Question clues towards Alzheimer’s disease: memory changes first before personality. As night progresses they are unable to sleep. They would also have difficulty in daily tasks and be confused.
Vascular dementia would have a “stepwise progression” and they would have had some sort of previous cardiovascular event in the stem.
Lewy body dementia would require a clue into having Parkinsonian symptoms and hallucinations.
Normal pressure hydrocephalus presents with gait disturbance, urinary incontinence, and confusion.
Q.117. An 86 year old man was brought in by the police to the emergency department after being found wandering the streets in the middle of the night outside his home. He has been living alone since his wife died a year ago. The police had recorded accounts from neighbours that had reported him to have had increased forgetfulness and requiring help to get back home in the past eight to nine months. When neighbours have found him at times, they report that he has been talking to himself. What is the most likely diagnosis?
Correct Answer : C
This gentleman likely had some cognitive impairment when his wife was alive. She likely helped him with his day-to-day activities. Therefore the problems likely did not surface.
Now that he has no support, his impairments have likely worsened and he has not been able to manage alone. Orientation to time is usually lost first typically in dementia, followed by an orientation to place, and finally to person when it is most severe.
Q.118. A 45 year old man presents to the emergency department with acute back pain radiating down to his legs, urinary retention and incontinence. On examination, perineal sensory loss is noted. What is the most appropriate investigation?
Correct Answer : A
This is a classic example of cauda equina syndrome.
It is a serious neurologic condition in which damage to the cauda equina causes loss of function of the nerve roots of the spinal canal below the termination (conus medullaris) of the spinal cord. Any lesion which compresses or disturbs the function of the cauda equina may disable the nerves although the most common is a central disc prolapse. Investigation of choice is an MRI.
Q.119. A 52 year old man has incoherent speech. He is aware of his speech difficulties but finds difficulty in using the right words when speaking. He has no other symptoms apart from his speech issue. He has good comprehension. Which anatomical site is most likely to be affected?
Correct Answer : C
Broca’s Aphasia - Broca’s area is a region in the inferior frontal lobe of the dominant hemisphere responsible for speech production. Lesions in this area produce a non-fluent or expressive aphasia. Patients will typically exhibit slow and halting speech. However, their comprehension is not affected.
Unlike Wernicke’s aphasia, patients with Broca’s aphasia are aware of their language difficulties.
For example, a person with Broca's aphasia may say slowly something like, "Bathe. Dog" meaning to say, "I bathe the dog today". You can see that the content of the information is correct, but the grammar and fluidity of the sentence are incorrect. They know what to say, they just cannot get it out.
Q.120. A 26 year old man complains of leg weakness. He first felt pins and needles on his feet which was followed by weakness of his legs for the past 2 days. He describes himself as a fit man who goes jogging every day however he now finds himself with great difficulty trying to stand due to his leg weakness. He gives a history of feeling unwell and having flu-like symptoms last week which has resolved after a few days. On examination, he has mild bilateral facial weakness, reflexes are diminished and has impaired sensation in his legs. What is the most likely diagnosis?
Correct Answer : D
The symptoms here are classic for Guillain-Barre syndrome. The weakness progresses quickly and always begins in the lower limbs. There is usually a history of a respiratory or gastrointestinal infection preceding these symptoms.
Q.121. A 62 year old man has recently had a flu-like illness. He woke up with difficult and unclear articulation of speech. Movement of his eyelids and lips are weak on the right side. What is the most likely anatomical defect?
Correct Answer : A
Viral infection may cause facial nerve palsy.
Facial Nerve Palsy Presentation :
Weakness of the muscles of facial expression and eye closure. The face sags and is drawn across to the opposite side while smiling. Voluntary eye closure may not be possible and can produce damage to the conjunctiva and cornea. In severe cases, dysarthria and difficulty with eating may occur.
Q.122. A 73 year old woman presents to clinic accompanied by her son with a 6 month history of anorexia and altered bowel habits. She has no significant past medical history and is on aspirin. On examination, the patient has an expressionless face, she takes many steps to turn, has resting tremor predominantly in her right hand, and cogwheel rigidity. Cognition is intact. What is the most likely diagnosis?
Correct Answer : B
The clinical examination above is classic of Parkinson’s Disease :
Bradykinesia, rigidity, resting tremor, and postural instability. While the beginning of the case stem may point to possible malignancy, the examination results point to option D.
Parkinson’s disease: > 65 years.
Classic presentation on examination: Bradykinesia, rigidity, resting tremor, and postural instability - +/- Extra-neurological features
Diagnosis: Clinical diagnosis
Treatment: Referral to a neurologist before starting pharmacological management - Levodopa (gold standard).
Q.123. A 46 year old chronic alcoholic man is brought to the emergency department in a drowsy state. He is responding vaguely to questions. He denies any alcohol intake today. He walks with an ataxic gait. Examination reveals spontaneous upbeat nystagmus and hyperreflexia Haemoglobin 128 g/L Mean cell volume (MCV) 99 fL What is the most likely cause for his cognitive impairment?
Correct Answer : C
Although folate deficiency is more common in people who regularly misuse alcohol this is not the answer in this stem. A haemoglobin of 128 g/L is barely enough to cause any symptoms of anaemia. This man is suffering from Wernicke’s encephalopathy.
Eye-movement abnormalities seen in Wernicke’s encephalopathy include gaze-evoked nystagmus, spontaneous upbeat nystagmus, and horizontal or vertical ophthalmoplegia.
Wernicke's encephalopathy is a neuropsychiatric disorder caused by thiamine deficiency which is most commonly seen in alcoholics.
A classic triad of confusion, ophthalmoplegia, and ataxia may occur.
Treatment is with urgent replacement of thiamine (vitamin B1). If not treated Korsakoff's syndrome may develop as well.
This is termed Wernicke-Korsakoff syndrome and is characterized by the addition of Antero- and retrograde amnesia and confabulation in addition to the above classic triad.
Q.124. A 73 year old female patient presents with right sided hemiplegia and aphasia in the Emergency Department. Thee symptoms began in the morning and resolved spontaneously within 6 hours. An EEG conducted in the hospital revealed atrial fibrillation. What is the best scoring method to assess her risk for future stroke in the next week?
Correct Answer : D
You may have difficulty in choosing either ABCD2 or CHA2DS2-VASc as the answer but remember that in this case stem, they are asking for a risk of stroke in the next few days. ABCD2 score would be more appropriate.
Q.125. A 19 year old female with previous history of repeated pain over the medial canthus and chronic use of nasal decongestants, presents with abrupt onset of a severe headache, fever with chills and rigor, diplopia on lateral gaze, moderate proptosis and chemosis. On examination optic disc is congested. Which of the following is the most likely diagnosis?
Correct Answer : B
This case stem is rare to appear in exam, but knowing the presentation of how the question will appear differentiates it from options B, C, and E which occur more frequently in the exam. Cavernous sinus thrombosis can appear as an option to those questions.
Cavernous sinus thrombosis :
- Headache
- can be severe intensity
- Chemosis, oedematous eyelids, proptosis, painful ophthalmoplegia
- Fever
- Usually preceded by sinusitis
Diagnosis: CT/MRI venography
Treatment:
- Referral to neurosurgery
- Antibiotics
- Anticoagulation : heparin
- +/- Corticosteroids and surgical drainage.
Q.126. A 58 year old man presents with unsteadiness, difficulty walking and slurred speech. He has a history of hypertension and hypercholesterolaemia. He denies alcohol use. A stroke is suspected. What is the most appropriate investigation?
Correct Answer : B
Ataxia and slurred speech are features of the cerebellar lesion. Posterior fossa lesions are best imaged using magnetic resonance imaging.
A CT head would be the correct answer if asked about the best initial investigation to ensure there is no haemorrhage. Brain PET has limited clinical use.
Q.127. A 45 year old man, with no known medical illnesses, presents to the clinic with left facial pain for the past month. It is a sharp shooting pain that radiates around his left cheek while chewing. It would last a few seconds repeatedly throughout the day. He has taken ibuprofen but with no relief. On examination: blood pressure is 120/70 mmHg, neurological exam is normal, palpation to the left jaw and cheek elicits pain although jaw muscles are of full strength. What is the most appropriate management for this condition?
Correct Answer : D
Please see Q-68
Q.128. A 26 year old woman complains of headache of 1 day duration that has been intensifying in severity over the last few hours. There is discomfort while turning her head and cannot tolerate bright lights. On examination, there is no papilloedema nor rashes. Kernig’s sign is negative. Lumbar puncture results reveal: elevated protein, normal glucose, and lymphocytosis. She is generally unwell but haemodynamically stable. What is the most likely diagnosis?
Correct Answer : B
Know the types of meningitis since it overlaps with quite a few topics on the exam. Pay particular attention to the lumbar puncture results to differentiate each. Kernig’s sign does not need to be present for it to be a diagnosis of meningitis.
If you forget the lab results, look at the history: viral meningitis has less severe symptoms than bacterial meningitis which can progress rapidly and produce signs of septic shock.
TB meningitis is more gradual with fever, weight loss, and headache with progression to focal deficit & altered consciousness.
Presentation :
• Classic: headache, fever, photophobia, neck stiffness
• Cranial palsies: CN III, IV, VI, VII
Diagnosis:
Lumbar puncture :
• Normal or high CSF pressure
• Increased lymphocytes
• Elevated protein
• Glucose normal
Treatment :
• Regardless of whether meningitis is bacterial, viral, or TB as a cause - Give antibiotics before performing CT brain and lumbar puncture.
• If no rash: IV cefotaxime or IV ceftriaxone + IV vancomycin + IV ampicillin
• If raised intracranial pressure: Give mannitol.
Q.129. A 62 year old woman comes with complaints of drooping of both upper eyelids and painless double vision that she first noticed when reading. The drooping of eyelids keeps alternating between her right and left eye and is worse towards the end of the day. Her speech is noted to be gradually getting slower and softer towards the end. Her pupils are normal on examination. The visual acuities are 6/6 in either eye. Which investigation will help in confirming the diagnosis?
Correct Answer : C
The woman has presented with features of myasthenia gravis. Almost all patients with myasthenia gravis will have ocular manifestations at some point during their disease. The most important feature is that muscles fatigue more readily after exercise.
Antibodies to acetylcholine receptors are seen in 85-90% of cases hence the answer is serum skeletal muscle nicotinic acetylcholine receptor antibody. Tensilon test is not routinely done any longer.
MYASTHENIA GRAVIS :
• Female (20-30 years); males (50-60 years)
• Painless muscle weakness that increases with exercise. This feature of fatigue often gives the diagnosis in the exam.
- It is even seen in the voice. For example, getting the patient to count up to 50. As the patient nears 50 their voice becomes less audible as they are fatiguing.
• Ocular muscles involved, drooping eyelids
• Dysphagia, dysarthria, dysphonia
• Normal reflexes
• Associated with hyperthyroidism
A useful mnemonic to remember for clinical features of myasthenia gravis is “D”.
• Diplopia
• Drooping eyelids
• Dysphagia
• Dysarthria
• Dysphonia
Q.130. A 48 year old male patient presents with symptoms of generalised muscle weakness, nausea, vomiting, polyuria and polydipsia. He was diagnosed with liver carcinoma three months ago. An MRI was done not too long ago and it was discovered that he now has brain metastasis. On examination, he is lethargic and has diminished deep tendon reflexes. Baseline blood tests have been done and show: Serum sodium: 147 mmol/L Serum potassium: 4.2 mmol/L Urea 4.4 mmol/L Creatinine: 89 micromol/L Chloride: 102 mmol/L Where is the most likely area of lesion?
Correct Answer : D
The best answer in the choices that fits in with this patient’s signs and symptoms is diencephalon.
The diencephalon consists of the thalamus, the hypothalamus including the posterior pituitary, the epithalamus, and the subthalamus. A lesion near or at the posterior pituitary would give rise to this patient’s symptoms of diabetes insipidus. The signs and symptoms of sodium imbalance are primarily neurological.
Q.131. A 61 year old female is brought to the hospital by her daughter following a drastic change in her behaviour. Her daughter says that her mother’s behaviour began to change three days ago whereby she became restless and aggressive. The daughter describes going to visit her mother three days ago and getting complaints from the neighbours that they hear banging and shouting all night. The patient herself claims that there are people who enter her room at night and she makes those noises to scare them off. There is no evidence to back up the patient’s claims. What is the most likely diagnosis for her condition?
Correct Answer : D
Delirium describes an acute confusional state and is very common in the elderly. It involves altered perception and thought and is of acute onset. The other answers are less likely.
Dementia is incorrect as a person with dementia would have a chronic set of symptoms and a slow decline in mental functioning over a long period. Mania describes an elevated mood.
This can present as an abnormally high level of arousal or energy.
This patient does not present with any of those symptoms. Schizophrenia is less likely as a majority of schizophrenics develop their symptoms around adolescence or early adulthood. This patient is 61 years old. Bipolar disorder presents with alternating episodes of hypomania and depression.
Q.132. A 19 year old woman complains of episodic headaches preceded by fortification spectra. These episodes can sometimes last for 2-3 days. When these headaches occur, she prefers to be in a quiet, dark room. What is the most appropriate management for the acute phase?
Correct Answer : A
The diagnosis here is migraine.
This question is a helpful reminder that the mean age of onset of migraines is 19 years old. It is usually a young to middle-aged person who presents with migraines. It is highly unlikely that they would ask you to choose between an oral triptan, NSAID, aspirin, or paracetamol for the acute treatment of migraines.
Q.133. A 70 year old woman was brought into the Emergency Department by her son for increasing confusion and slurred speech. On examination, she was oriented to time, place and person. Neurological examination was positive for bilateral past pointing and truncal ataxia but no nystagmus. Blood tests were within normal limits. Where is the most likely location of her lesion?
Correct Answer : B
Stroke questions come in various forms ranging from the anatomical locations of the lesion to investigations and management. Pay special attention to the anatomy of the lesions especially the vascular distribution and the functions of the different parts of the brain.
Key clues to cerebellum lesions: dysdiadochokinesia, ataxia, nystagmus, intention tremor, slurred speech, hypotonia, past pointing.
Q.134. A 45 year old man has been admitted for an elective surgery. 2 days later he develops agitation, sweating and complains of seeing snakes on the hospital wall. A history of chronic alcoholic abuse is revealed and chlordiazepoxide has been started. What is the most appropriate next course of action?
Correct Answer : D
In regards to his diagnosis of chronic alcoholic abuse, add thiamine to the mix to prevent Wernicke’s encephalopathy even though he is not showing any signs of Wernicke’s encephalopathy.
Parenteral thiamine should be prescribed for treatment of suspected or confirmed Wernicke’s encephalopathy, and for prophylaxis in alcohol-dependent patients attending the hospital for acute treatment.
Q.135. A 40 year old woman suddenly collapsed and died. At the post-mortem autopsy, it was found that there was a bleed from a berry aneurysm from the circle of Willis. Which is the most likely space that the bleeding occurred in?
Correct Answer : A
Subarachnoid haemorrhage (SAH) is spontaneous in the context of a ruptured cerebral aneurysm but may be seen in association with other injuries when a patient has sustained a traumatic brain injury. Aneurysm formation is the most common aetiology.
There is also an association with polycystic kidney disease, Ehlers-Danlos syndrome, and another connective tissue disease. Head trauma is rare as a cause of SAH.
Q.136. A 42 year old man has increasing daytime sleepiness. He feels that his tiredness is affecting his work as he is unable to keep awake during meetings. He also complains of choking episodes during his sleep. On examination, his BMI is 36 kg/m2, blood pressure is 150/70 mmHg, and respiratory exam was normal. What is the most likely diagnosis?
Correct Answer : B
Daytime sleepiness and obesity point to the diagnosis of obstructive sleep apnoea syndrome. Choking episodes during sleep are also a suggestive feature of obstructive sleep apnoea syndrome.
Obstructive sleep apnoea syndrome :
- Middle-aged to elderly male
- Increased daytime sleepiness, fatigue, sleep disruption
- Snoring loudly at night
- Associated with hypertension, diabetes, obesity
Diagnosis:
- Pulse oximetry, overnight study of breathing pattern (initial investigation)
- Polysomnography (gold standard)
Treatment:
- Conservative: weight loss and reduced alcohol consumption
- Continuous positive airway pressure (CPAP).
Q.137. A 41 year old male with hypertension and recurrent kidney stones presents to the Emergency Department with a headache of intense severity. He is also noted to have neck stiffness and pain. Labs were done and revealed a serum sodium of 131 mmol/L. What is the most likely mechanism behind his sodium results?
Correct Answer : B
This is a 2 step question. First figure out the diagnosis and through that find out the answer to the question. Some questions will require you to do this.
In this case, the diagnosis is subarachnoid hemorrhage (SAH) and it is also implied in the case stem that the patient has possible polycystic kidney disease (hypertension and recurrent kidney stones).
One of the major complications of SAH is hyponatremia.
Hyponatremia commonly occurs in patients with aneurysmal subarachnoid haemorrhage. The mechanism that has been proposed as a cause is the syndrome of inappropriate anti-diuretic hormone.
Q.138. A 45 year old man has acute back pain radiating down to his legs and faecal incontinence. On examination, perineal sensory loss is noted. What is the most likely diagnosis?
Correct Answer : C
Cauda Equina Syndrome would fit the best. Although lumbosacral disc herniation and degenerative process of the spine are causes of cauda equina syndrome it would be more accurate to put Cauda Equina Syndrome as the answer due to the perineal sensory loss.
Cauda Equina Syndrome is a serious neurologic condition in which damage to the cauda equina causes loss of function of the nerve roots of the spinal canal below the termination (conus medullaris) of the spinal cord.
Q.139. A 78 year old smoker collapses and is brought into accident and emergency. He is unable to lift his right hand or leg. He also complains of double vision. His left pupil is mydriatic and his left eyelid droops downowards. His left eye is deviated downwards and outwards. He is a known diabetic and has a history of hypertension. Where is the most likely area of the lesion?
Correct Answer : A
This male has most likely suffered a midbrain infarct. This specific presentation is called Weber’s syndrome which is a result of a midbrain infarct. It is a form of stroke characterized by the presence of:
1. Contralateral hemiparesis
2. An ipsilateral oculomotor nerve palsy
Q.140. A 43 year old man presents with neck stiffness, headache and vomiting. The headache is severe, persistent and on the left side. He also has ear pain and discharge coming from his left ear. On examination, he has weakness of the right hand and leg. He has a temperature of 38.5 C. What is the most likely diagnosis?
Correct Answer : D
CEREBRAL ABSCESS : Cerebral abscesses may show many of the same features of brain tumors as they both are space-occupying lesions. The major difference is that cerebral abscess has features of a fever and an obvious source of infection nearby such as otitis media or mastoiditis.
Presentation :
• Headache is the most common symptom and it is often on the same side as the abscess
• Fever
• Changes in mental state (drowsiness, confusion)
• Focal neurological deficits
• Grand mal seizures
• Nausea and vomiting
• Neck stiffness
• Papilloedema, this is due to cerebral oedema
Investigations :
• CT scanning is the investigation of choice. Cerebral abscesses appear as a radiolucent space-occupying lesion.
Q.141. A 28 year old woman has a short history of double vision. She tires easily, especially as the day progresses. There is difficulty climbing stairs, reaching for items on shelves, and brushing her hair. As she speaks, her speech fades gradually. Over the last week, she has had difficulty chewing and swallowing. On examination, there were no significant findings. She has a family history of thyroid disease. What is the most likely diagnosis?
Correct Answer : C
The symptoms here are classic for Myasthenia gravis. It is important to remember that there is a predisposition for autoimmune diseases to run in families hence the history of thyroid disease in the family in the stem.
Q.142. A 30 year old presents to the emergency department with confusion and ataxia. She had a surgical abortion 3 days ago at 13 weeks gestation. Her pregnancy was complicated with severe hyperemesis gravidarum. On examination, she has horizontal ophthalmoplegia. She is unsteady and has uncoordinated walking. She denies alcohol intake. What is the most appropriate management?
Correct Answer : A
She is suffering from Wernicke’s encephalopathy. One of the eye abnormalities seen in Wernicke’s encephalopathy is horizontal or vertical ophthalmoplegia.
Wernicke’s encephalopathy is a neuropsychiatric disorder caused by thiamine deficiency which is most commonly seen in alcoholics. A classic triad of confusion, ophthalmoplegia, and ataxia may occur.
It is also seen in pregnancy where there is severe persistent hyperemesis gravidarum.
For this reason, it is important to replace thiamine in patients with hyperemesis gravidarum before they develop Wernicke’s encephalopathy.
Treatment in this case is with urgent replacement of thiamine (vitamin B1).
Wernicke’s Encephalopathy triad of:
1. Confusion
2. Ataxia
3. Ophthalmoplegia
Q.143. A 75 year old nursing home resident complains of worsening headache, and impaired vision for 4 days. Her daughter says she is getting more and more confused day by day. She has multiple bruises on her head. What is the most likely cause of her confusion?
Correct Answer : D
Among the given answers, subdural haematoma fits the best. The multiple bruises on her head suggest head injury which can lead to subdural haematoma. Headache, confusion, and impaired vision for 4 days could occur in chronic subdural haematoma. She is an elderly lady thus a trivial fall may have gone unnoticed.
Q.144. A 63 year old man, known case of hypertension and smoker, presents to clinic with a sudden onset of weakness in the right arm and changes in speech which had resolved within a 24 hour period. On examination, there were no residual neurological findings and cardiology examination was normal. What is the most appropriate next step in management?
Correct Answer : C
This is a classic presentation of a transient ischaemic attack. Under the ABCD2 score, this patient has a score of 4. The most appropriate step according to guidelines is for carotid doppler scanning to check for carotid artery stenosis to assess the need for carotid endarterectomy.
MRI would eventually be done but it would not be the “next step” as the patient no longer has residual neurological findings and his symptoms have completely resolved; therefore MRI at this moment would not be clinically beneficial.
Q.145. A 33 year old woman with multiple sclerosis complains of vertigo and double vision. She has also noticed recent drooping of her lips on the left side. She has loss of sensation over her face, reports intermittent shooting pains over the face and has increasing difficulty with hearing. She has a lack of voluntary coordination of muscle movements. The symptoms have been worsening over the past 3 days. What is the most likely anatomical site affected?
Correct Answer : A
Plaques can develop anywhere in the central nervous system in patients with multiple sclerosis, but when they develop in the brain stem, several functions can be impaired and may result in an evolving vestibular syndrome. Vertigo is often seen with diplopia due to the demyelination of cranial nerves III, IV, and VI as they leave the brainstem in patients suffering from multiple sclerosis.
Q.146. A 72 year old woman presents with the complaint of forgetfulness for three months. She used to live with her husband but since his passing four months ago, has been living alone. For the past three months, she has been increasingly forgetful and more socially withdrawn. She contacts her children less frequently than she used to and has been late in paying her bills. She blames her recent memory impairment on tiredness. Her medical history includes having depression more than 20 years ago. What is the most likely diagnosis?
Correct Answer : D
PSEUDODEMENTIA: Severe depression that presents with poor memory and concentration and impaired functional capacity. Seen in elderly patients whereby they exhibit symptoms consistent with dementia but the cause is depression.
Features- Onset relatively abrupt, Poor memory, Often with a history of depression. If asked questions, would reply “I don’t know, I can’t be bothered, it’s too difficult” (This is because they are often upset but their attention and concentration are often intact)
Response to antidepressant medication.
Q.147. A 38 year old male presented to Accident and Emergency with the complaint of bilateral lower limb weakness. He said that he first noticed this two days ago when he fumbled while walking down the stairs. He has been noticing a gradual increase in muscle weakness of his legs and he is now unable to walk at all. The patient mentions an episode of diarrhoea that began one week ago and that lasted approximately two days. He works as a shop assistant and reports no problems at home or at work. The patient was subsequently admitted to the medical ward and physical examination of his limbs revealed a loss of deep tendon reflexes. His bilateral leg paralysis has now ascended to affect both of his upper limbs as well. What is the most likely mechanism causing this patient’s problems?
Correct Answer : C
The patient has Guillain-Barre syndrome. Clues that allude to this diagnosis include his symptoms of ascending limb weakness accompanied by hyporeflexia as well as his history of a recent illness.
Guilllain-Barre syndrome is a disorder whereby antibodies created by the body to attack infectious organisms (usually of the gastrointestinal or respiratory tract) also attack antigens in the peripheral nerve tissue.
The major complaint in most patients is weakness or neuropathic pain.
Q.148. A 44 year old man presents to Emergency after falling from a third floor building. His Glasgow Coma Scale is 4/15. He is intubated and ventilated on arrival. Neurological examination reveals unequal pupils. CT head and neck reveals midline shift and a left-sided convex enhancing area. What is the most appropriate action?
Correct Answer : A
This is a diagnosis of extradural haemorrhage. While this is a frequent neurology topic, the presentation here has left out the usual clue: “lucid interval”. However, the stem provides another clue to the diagnosis: the CT findings which are indicative of an extradural haemorrhage.
In this case, this patient not only has raised intracranial pressure but he is also showing signs of neurological deficit (unequal pupils) in addition to the low GCS.
Therefore, he is not suitable for conservative management and requires immediate craniotomy for evacuation of the haematoma.
Q.149. A 51 year old male with a Pancoast tumour presents with unilateral partial ptosis, anhidrosis and miosis on the right side of his face. What is the most likely underlying mechanism for the syndrome?
Correct Answer : D
This man is suffering from Horner’s syndrome secondary to the Pancoast tumour. Horner’s syndrome describes an ipsilateral deficiency of sympathetic activity. There are many causes of Horner’s syndrome, but the one that is tested the most in exams is a Pancoast tumour.
Q.150. A 79 year old man presents to the Emergency Department with an acute onset of double vision and vertigo. He has paraesthesia of his upper limbs. He is becoming increasingly drowsy with an unsteady gait. What is the most likely diagnosis?
Correct Answer : C
A significant differential when a patient presents to the Emergency Department with acute vertigo accompanied by neurological symptoms is brain stem and cerebellar strokes. Brain stem strokes have complex symptoms and are difficult to diagnose.
The hallmarks of brain stem strokes are symptoms of vertigo, ataxia, and diplopia.
Other symptoms include slurred speech, numbness of the face, and decreased level of consciousness. The distractor is cerebellar strokes.
Cerebellar infarcts also present with acute vertigo. If the inferior cerebellum is affected, in addition to vertigo, patients could have nystagmus and postural instability however a pure cerebellar stroke would not usually have limb paraesthesia or diplopia.
Q.151. A 72 year old woman who is in long-term residential care has recently become deliriouis and distressed following a chest infection. She has already been prescribed antibiotics for the chest infection which she started taking a day ago. The staff are concerned that she is a risk to herself. They have attempted verbal and non-verbal de-escalation techniques however she continues to be agitated and restless. What is the most appropriate short-term medication?
Correct Answer : B
NICE has suggested short-term olanzapine or haloperidol (usually for a week or less) be used in patients with delirium who are in distress once non-pharmacological de-escalation techniques have failed.
Q.152. A 67-year-old man after a stroke, presents with left sided ptosis and constricted pupil. He also has loss of pain and temp on the right side of his body and left side of his face. Which part of the brain is most likely affected?
Correct Answer : D
The name of the condition is “Lateral medullary syndrome”.
Lateral medullary syndrome is a neurological disorder causing a range of symptoms due to ischemia in the lateral part of the medulla oblongata in the brainstem. The ischemia is a result of a blockage most commonly in the vertebral artery or the posterior inferior cerebellar artery.
This syndrome is characterized by sensory deficits that affect the trunk and extremities contralaterally and sensory deficits of the face and cranial nerves ipsilaterally.
Specifically, a loss of pain and temperature sensation if the lateral spinothalamic tract is involved. The cross-body finding is the chief symptom from which a diagnosis can be made (in short ipsilateral Horner syndrome and contralateral loss of pain and temperature sense).
The patient may have ataxia (cerebellar involvement), dysphagia (nucleus ambigus that involves vagus and glossopharyngeal nerve dysfunction), and slurred speech. Vestibular nuclei dysfunction may cause vomiting, vertigo, and nystagmus.
Q.153. An 18-year-old female has peri-orbital blisters. Some of them are crusted, others secreting pinkish fluid. What is the most likely diagnosis?
Correct Answer : A
Herpes zoster ophthalmicus occurs when the varicella-zoster virus is reactivated in the ophthalmic division of the trigeminal nerve. Herpes zoster is a common infection caused by the human herpesvirus 3, the same virus that causes varicella (i.e., chickenpox).
Q.154. A 22-year-old man has a reduced conscious level and a fixed dilated pupil after being involved in a MVC (motor vehicle collision). Choose the most appropriate option?
Correct Answer : B
3rd nerve damage can cause fixed dilated pupil.
Q.155. A-7-year old child is brought to the emergency department with a 1 day history of being listless. On examination, the child is drowsy with an extensive non-blanching rash. What advice would you give the parents?
Correct Answer : D
Diagnosis is meningococcal meningitis. All contacts need rifampicin prophylaxis.
Q.156. A patient was lying down on the operating table in a position with his arms hanging down for 3 hours. Soon after he woke up, he complains of numbness and weakness in that hand and has limited wrist movement/wrist drop and sensory loss over dorsum of that hand, weakness of extension of the fingers and loss of sensation at the web of the thumb. What structure is likely to be damaged?
Correct Answer : A
Here arm hanging down compressing the radial nerve at the spiral groove is the cause of the given scenario.
Q.157. A 65-year-old woman presented with transient arm and leg weakness as well as a sudden loss of vision in the left eye. Her symptoms resolved within the next couple of hours. What is the most appropriate next investigation?
Correct Answer : C
Diagnosis is TIA. The probable cause is carotid narrowing from atherosclerosis.
Q.158. A man complains of loss of sensation in his little and ring finger. Which nerve is most likely to be involved?
Correct Answer : B
Compression of ulnar nerve at the elbow, known as cubital tunnel syndrome, causes numbness in the 5th finger, along the half (lengthwise) of the 4th (ring) finger closest to the 5th finger, and the back half of the hand over the 5th finger.
Q.159. A young man complains of double vision on seeing to the right. Which nerve is most likely to be involved?
Correct Answer : B
Diplopia on seeing to the right indicates right lateral rectus palsy which is supplied by the right abducent nerve.
Q.160. A patient with cerebral metastasis has polyuria and polydipsia. Which part of the brain is affected?
Correct Answer : C
Diencephalon is the caudal (posterior) part of the forebrain, containing the epithalamus, thalamus, hypothalamus, ventral thalamus, and the third ventricle. The hypothalamus produces ADH and hens lesion of the diencephalon (hypothalamus) may produce cranial diabetes insipidus.
Q.161. A-45-year old female complains of pain in the inner side of her right thigh. She was diagnosed with benign ovarian mass on the right. Which nerve is responsible for this pain?
Correct Answer : B
The Obturator nerve is responsible for the sensory innervation of the skin of the medial aspect of the thigh.
Q.162. A 79-year-old stumbled and sustained a minor head injury 2 weeks ago. He has become increasingly confused, drowsy and unsteady. He has a GCS of 13. He takes warfarin for Atrial fibrillation. What is the most likely diagnosis?
Correct Answer : D
In the elderly head injury usually leads to subdural hematoma even if a head injury is minor or trivial and extradural hematoma in the elderly is extremely uncommon even in more severe head injury. Warfarin is also a risk factor for subdural hematoma from a minor trauma.
Management:
1st line: Evacuation by barr hole craniostomy.
2nd line: Craniotomy if the clot is organized. Up to 3 weeks burrhole may be possible but longer than this clot is mostly organized and Flap craniotomy is usually required.
Q.163. A 22-year-old lady has been unwell for some time. She came to the hospital with complaints of fever and painful vesicles in her left ear. What is the most probable diagnosis?
Correct Answer : B
This is a case of Herpes zoster oticus and if the facial nerve is also involved then it is called Ramsay Hunt syndrome.
Q.164. A 62-year-old woman complains of unsteadiness when walking. On examination she has pyramidal weakness of her left lower limb and reduced pain and temp sensation on right leg and right side of trunk up to the umbilicus. Joint position sense is impaired at her left great toe but is normal elsewhere. She has a definite left extensor plantar response and the right plantar response is equivocal. Where is the lesion?
Correct Answer : D
In Brown-Sequard syndrome paralysis and loss of proprioception on the same (or ipsilateral) side as the injury or lesion, and loss of pain and temperature sensation on the opposite (or contralateral) side as the lesion.
Q.165. A woman has electric pains in her face that start with the jaw and move upwards. Her corneal reflexes are normal. What is the most likely diagnosis?
Correct Answer : B
Trigeminal neuralgia.
Electric pains in her face that start with the jaw and move upwards this description indicates neurological pain of the trigeminal nerve. Patients with classical trigeminal neuralgia have a normal neurologic examination.
Sensory abnormalities in the trigeminal area, loss of corneal reflex, or evidence of any weakness in the facial muscles should prompt the physician to consider symptomatic trigeminal neuralgia or another cause of the patient's symptoms.
Q.166. A 56-year-old man comes with history of right sided weakness & left sided visual loss. Where is the occlusion?
Correct Answer : D
Carotid artery divides into internal and external carotid of which the internal continues as middle cerebral ultimately.
But just before it becomes middle cerebral internal carotid gives rise to ophthalmic branch. So middle cerebral occlusion may give partial visual loss but not complete mono-ocular blindness.
For complete mono-ocular blindness occlusion should be proximal to the ophthalmic artery i.e. either in the internal carotid or more proximally to the carotid artery.
Q.167. A 24-year-old college student presents with nausea, vomiting, headache, neck stiffness and a fever of 38.4C. What is the most appropriate empirical antibiotic to be started?
Correct Answer : A
Empiric therapy should begin as soon as bacterial meningitis is thought likely. In patients with meningitis caused by penicillin- or cephalosporin-resistant strains, vancomycin may be used in combination with a third-generation cephalosporin but should not be used alone.
Though meropenem can be an alternative to cefotaxime and ceftriaxone due to its seizure activity it is not preferred as 1st line. Fluoroquinolones are also not used as 1st line.
Q.168. A 56-year-old lady has developed severe right sided headache which worsens whenever she comes to bright light since the last 4 days. She feels nauseated, but doesn’t vomit. What is the most likely diagnosis?
Correct Answer : C
This is migraine with aura. Criteria of migraine without aura:
5 headaches + nausea/vomiting or photophobia + any 2 of:
i) unilateral
ii) pulsating
iii) worsen by routine activity
Q.169. A 33-year-old male involved in a street fight presents with bruises and deformity in the upper part of his leg. X-ray shows fracture of the neck of fibula. What is the single most associated nerve injury?
Correct Answer : D
Lateral peroneal nerve is another name for superficial peroneal nerve.
Q.170. A 37-year-old man slipped while he was walking home and fell on his out stretched hand. He complains of pain in the right arm. X-ray showed fracture of the head of radius. What is the most associated nerve injury?
Correct Answer : A
Radial nerve
Q.171. A 53-year-old woman presented with pain in the eye, blurry vision and clumsiness for 3 months. She has a history of difficulty in swallowing and weakness in her right upper limb 2 years ago. What is the investigation of choice?
Correct Answer : D
Diagnosis is multiple sclerosis for which MRI is the investigation of choice.
Q.172. A 44-year-old patient comes with right hemiparesis. Examination: left sided ptosis and left dilated pupil. Where is the lesion?
Correct Answer : D
The diagnosis is Weber syndrome which is characterized by presence of ipsilateral oculomotor nerve palsy and contralateral hemiparesis or hemiplegia.
Q.173. A 30-year-old woman has brief episodes of severe shooting pain in the rectum. Rectal examination and flexible sigmoidoscopy are normal. What is the most probable diagnosis?
Correct Answer : C
Proctalgia fugax is a functional anorectal disorder characterized by severe, intermittent episodes of rectal pain that are self-limited. The diagnosis of proctalgia fugax requires the exclusion of other causes of rectal or anal pain. Normal rectal examination and flexible sigmoidoscopy exclude other options.
Q.174. A 23-year-old lady presents with headache. Examination: photophobia and generalized rash that doesn’t blanch on pressure. What must be done immediately?
Correct Answer : A
IV benzylpenicillin.
Likely diagnosis is meningococcal meningitis.
Q.175. A young girl complains of episodic headaches preceded by fortification spectra. Each episode last for 2-3 days. During headache patient prefers quiet, dark room. What is the treatment of choice for acute stage?
Correct Answer : A
Aspirin may cause Reye’s syndrome in young girls. This is a case of pediatric migraine (pediatric migraine up to 17yrs).
In pediatric migraine paracetamol is 1st line treatment (also ibuprofen). In pediatric migraine, the GP cannot prescribe triptan.
Q.176. A-33-year old man is hit by a car. He loses consciousness but is found to be fine by the paramedics. When awaiting doctors review in the ED he suddenly becomes comatose. What is the most likely diagnosis?
Correct Answer : D
Age 33 considerable head trauma, and lucid interval are the points in favour of extradural hemorrhage.
Q.177. A 77-year-old male presents with history of enuresis and change in behavior. Examination: waddling gait. What is the most likely diagnosis?
Correct Answer : C
Normal pressure hydrocephalus (NPH) is an abnormal buildup of cerebrospinal fluid (CSF) in the brain's ventricles or cavities.
It occurs if the normal flow of CSF throughout the brain and spinal cord is blocked in some way. This causes the ventricles to enlarge, putting pressure on the brain.
Age (usually occurs in the 60s or 70s), loss of bladder control (enuresis), waddling gait and behavior change, and dementia are all features of normal pressure hydrocephalus.
Q.178. A 17-year-old girl had an episode of seizure. Contraction of muscles started from around the interphalangeal joints, which spread to the muscles of wrist and elbow. Choose possible type of seizure?
Correct Answer : C
Myoclonus can be described as brief jerks of the body; it can involve any part of the body, but it is mostly seen in limbs or facial muscles. The jerks are usually involuntary and can lead to falls. EEG is used to read brain wave activity.
When myoclonic jerks are occasionally associated with abnormal brain wave activity, they can be categorized as myoclonic seizures. If the abnormal brain wave activity is persistent and results from ongoing seizures, then a diagnosis of myoclonic epilepsy may be considered.
Q.179. A 72-year-old man fell while shopping and hurt his knee. His vitals are fine. He speaks in a low voice and is very slow to give answers. What is the most probable diagnosis?
Correct Answer : A
Alzheimer's disease, is a chronic neurodegenerative disease that usually starts slowly and gradually worsens over time. It is the cause of 60–70% of cases of dementia. The most common early symptom is difficulty in remembering recent events.
As the disease advances, symptoms can include problems with language, disorientation (including easily getting lost), mood swings, loss of motivation, not managing self-care, and behavioural issues. As a person's condition declines, they often withdraw from family and society. Gradually, bodily functions are lost, ultimately leading to death.
Q.180. A 70-year-old man presents with balance difficulties, vomiting and nausea. Which of the following is the best investigation?
Correct Answer : A
Balance difficulties, vomiting and nausea suggests cerebellar lesion. In posterior fossa lesion MRI is preferred.
Q.181. A 78-year-old lady on warfarin for atrial fibrillation lives in a care home. She presents with history of progressive confusion for three days. She was also noticed to have bruises on her arms. INR 7. What is the most probable diagnosis?
Correct Answer : C
Age 78 yrs, living in a care home where the unnoticed trivial injury is possible (like fall), warfarin and high INR a potential risk factors of subdural haemorrhage suggested by bruises on arms also.
Q.182. A 32-year-old woman suffers an episode of severe occipital headache with vomiting and loss of consciousness. She is brought to the hospital where she is found to be conscious and completely alert. Examination: normal pulse & BP. No abnormal neurological signs. What is the next step in management?
Correct Answer : D
Basilar migraine can cause severe headaches and LOC.
The diagnostic criteria are those of migraine with aura, consisting of at least two of the following fully reversible symptoms, but no motor weakness: dysarthria, vertigo, tinnitus, hyperacusis, diplopia, and visual symptoms present simultaneously in both temporal and nasal fields of both eyes, ataxia, decreased level of consciousness, and simultaneously bilateral paresthesias.
Q.183. A 63-year-old female is noted to have left pupil irresponsive to light and is dilated. What is the most probably diagnosis?
Correct Answer : B
In the elderly extradural hemorrhage is unlikely and subdural hemorrhage is more common. Traumatic expanding subdural hematomas may present with third nerve involvement and are usually accompanied by additional neurological dysfunction.
Dilated, sluggish, or fixed pupil, bilateral or ipsilateral to the injury occurs due to increased intracranial pressure.
Q.184. A teacher brings in a child who says she fell down after hitting a table. On probing further, you decide that it was most probably an absence seizure. What led you to this diagnosis?
Correct Answer : B
The child suddenly went blank and there was up-rolling of eyes.
An absence seizure is a generalized onset seizure, which means it begins on both sides of the brain at the same time. An older term is petit mal seizures. Absence seizures usually affect only a person's awareness of what is going on at that time, with immediate recovery.
Q.185. A 74-year-old man presents with weakness in his arm and leg from which he recovered within a few days and short term memory loss. He has an extensor plantar response. He has similar episodes 2 years ago and became unable to identify objects and to make proper judgment. What is the most appropriate diagnosis?
Correct Answer : D
Vascular dementia.
Hemiparesis, memory impairment, extensor planter reflex, inability to identify objects, and poor judgment are features of strokes. So likely diagnosis is vascular dementia.
Q.186. A 70-year-old lady presents with fever for 3 days and confusion. There is no significant PMH (past medical history). What is the most probable diagnosis?
Correct Answer : A
Delirium is an acute confusional state and declined cognitively function which involves changes in arousal (hyperactive, hypoactive, or mixed), perceptual deficits, altered sleep-wake cycle, and psychotic features such as hallucinations and delusions.
Q.187. An obese mother suffers from OSAS (obstructive sleep apnoea syndrome). Which of the following investigation is best for her?
Correct Answer : B
This is already a diagnosed case of OSAS. So no need for reconfirmation with polysomnography. If like to know the current status or monitor overnight pulse oximetry is good.
Q.188. A 29-year-old woman who was diagnosed to have migraine presents with severe onset of occipital headache. She lost her consciousness. CT scan normal. Neurological examination normal. What is the most appropriate management?
Correct Answer : D
This is a case of basilar migraine. No investigation required.
Q.189. A 60-year-old woman was found by her son. She was confused and had urinary incontinence. She has recovered fully after 6hours with no neurological complaints. What is the most likely diagnosis?
Correct Answer : C
Stroke or transient ischemic attack (TIA) may be a risk factor for urinary incontinence.
Q.190. A 34 year-old-male presents with history of headache presents with ataxia, nystagmus and vertigo. Where is the site of the lesion?
Correct Answer : C
Features described are consistent with cerebellar lesion.
Q.191. A young girl presenting with fever, headache, vomiting, neck stiffness and photophobia. She has no rashes. What is the most appropriate test to confirm the diagnosis?
Correct Answer : C
Case of meningitis. LP will confirm the diagnosis.
Q.192. A 65-year-old hypertensive man wakes up in the morning with slurred speech, weakness of the left half of his body and drooling. Which part of the brain is affected?
Correct Answer : B
As symptoms are on left side lesion is on right side of the brain.
So answer should be either b) right internal capsule or c) right midbrain. If it was midbraine there would have cranial nerve involvement.
On the other hand given picture is very much consistent with lacunar infarction of internal capsule.
Q.193. A man presents with muffled hearing and feeling of pressure in ear with tinnitus and vertigo. He also complains of double vision when looking to the right. What is the most appropriate diagnosis?
Correct Answer : B
An acoustic neuroma (vestibular schwannoma) is a benign tumor that develops on the vestibular and hearing, or auditory (cochlear) nerves leading from the patient’s inner ear to the brain.
The pressure on the nerve from the tumor may cause hearing loss and imbalance, the feeling of pressure in the ear with tinnitus, and vertigo. Involvement of other cranial nerves may occur, as here right abducent nerve (double vision when looking to the right).
Q.194. A 12-year-old girl presented with tics, LOC (loss of consciousness), no residual sign and no post-ictal phase. EEG abnormality in temporal lobe. The girl had a rapid recovery. What is the most probably diagnosis?
Correct Answer : C
Seizures may be described as either partial (focal) or generalized. Partial seizures only involve a localized part of the brain, whereas generalized seizures involve the whole of both hemispheres. As there is loss of consciousness this is a partial complex seizer.
Often focal seizures may precipitate into a generalized seizer called partial generalized seizures (more accurately “secondarily generalized seizer”).
Q.195. A 68-year-old man gets repeated attacks of LOC and TIA. What is the most likely cause for this?
Correct Answer : D
Carotid artery stenosis.
Q.196. A child was admitted following a RTA (road traffic accident) with initial GCS=15. Then during the night the noticed GCS reduced to 13. What is the management?
Correct Answer : D
Probable intracranial haemorrhage.
Q.197. A 56-year-old woman with MS (multiple sclerosis) presents with drooping of the left side of her lips. She also has loss of sensation over her face, hearing impairment and some in -coordination of her movements. What is the most likely anatomical site affected?
Correct Answer : D
Features of 5, 7, 8th cranial nerve and cerebellar involvement are suggestive of brainstem lesion.
Q.198. A 72-year-old man has been on warfarin for 2 years because of past TIA and stroke. What is the most important complication that we should be careful with?
Correct Answer : A
Headache is the warning sign of hemorrhagic stroke.
Q.199. A 64-year-old man has presented to the emergency department with a stroke. CT shows no hemorrhage. ECG shows atrial fibrillation. He has been thrombolysed and he’s awaiting discharge. What prophylactic regimen is best for him?
Correct Answer : A
Atrial fibrillation: post-stroke- following a stroke or TIA warfarin should be given as the anticoagulant of choice.
Q.200. A 54-year-old man after a CVA (cerebrovascular accident) presents with ataxia, intention tremors and slurred speech. Which part of the brain has been affected by the stroke?
Correct Answer : D
Following are the common features of cerebellar lesion:
i) Ataxia
ii) slurred speech or dysarthria
iii) dysdiodokokinesis
iv) intention tremor
v) nystagmus
Q.201. A 40-year-old chronic alcoholic who lives alone, brought in the emergency department having been found confused at home after a fall. He complains of a headache and gradually worsening confusion. What is the most likely diagnosis?
Correct Answer : D
Subdural hematoma may be acute or chronic. Chronic symptoms may not be apparent for several days or weeks.
Symptoms of subdural hematomas are fluctuating levels of consciousness, ± insidious physical or intellectual slowing, sleepiness, headache, personality change, and unsteadiness.
Treatment:
Evacuation via burr hole - 1st line.
Craniotomy if the clot organized - 2nd line.
Q.202. A 64-year-old man presents with a history of left sided hemiparesis and slurred speech. He was absolutely fine 6 hours after the episode. What is the most appropriate prophylactic regimen?
Correct Answer : C
Clopidogrel 75mg.
Q.203. A patient had TIA (transient ishchemic attack) which he recovered from. He has a history of stroke and exam shows HR (heart rate) in sinus rhythm. He is already on aspirin 75mg and anti-hypertensive drugs. What other action should be taken?
Correct Answer : D
He who is already on aspirin needs no change in aspirin dose. Clopidogrel is now the drug of choice for secondary prevention in TIA but if someone is already on aspirin he should continue it at the same dose and should be considered to shift to clopidogrel in the next few visits.
So for the given case correct option is to add statin only.
Q.204. A 44-year-old man comes with history of early morning headaches and vomiting. CT brain shows ring enhancing lesions. What is the most appropriate option?
Correct Answer : C
Toxoplasmosis is a parasitic disease caused by Toxoplasma gondii.
This can cause damage to the brain (encephalitis) particularly in immunocompromised people, such as those with HIV/AIDS, those taking certain types of chemotherapy, or those who have recently received an organ transplant.
Q.205. A 65-year-old man with difficulty in swallowing presents with an aspiration pneumonia. He has a bovine cough and fasciculating tongue. Sometimes as he swallows food it comes back through his nose. Choose the most likely cause of dysphagia from the given options?
Correct Answer : A
Dysphagia, nasal regurgitation, fasciculating tongue these are features of bulbar palsy due to a lower motor neuronal lesion of IX-XII nerves.
Q.206. A 38-year-old female presents with sudden loss of vision but fundoscopy is normal. She had a similar episode about 1 year ago which resolved completely within 3 months. Examination: mild weakness of right upper limb and exaggerated reflexes. What is the most appropriate treatment?
Correct Answer : C
Sudden loss of vision, remission and relapse of optic neuritis and focal neurological symptoms and exaggerated reflexes all point towards multiple sclerosis. The treatment option is corticosteroids.
Q.207. A 64-year-old woman has difficulty moving her right shoulder on recovering from surgery of the posterior triangle of her neck. What is the most appropriate option?
Correct Answer : A
Accessory nerve lesion causes weakness of the trapezius muscle and can produce a drooping shoulder, winged scapula, and weakness of forward elevation of the shoulder.
Q.208. A 50-year-old woman presents following a fall. She reports pain and weakness in her hands for several months, stiff legs, swallowing difficulties, and has bilateral wasting of the small muscles of her hands. Reflexes in the upper limbs are absent. Tongue fasciculations are present and both legs show increased tone, pyramidal weakness and hyper-reflexia with extensor plantars. Pain and temp sensation are impaired in the upper limbs. What is the most likely diagnosis?
Correct Answer : C
In MS there are characteristic relapse and remission which is absent here; In MND there is no sensory deficit;
Syringomyelia doesn’t cause cranial nerve lesions and in myasthenia, there is muscular weakness without atrophy. Here the features described well fit with syringobulbia.
Q.209. A 56-year-old man has symptoms of sleep apnea and daytime headaches and somnolence. Spirometry shows a decreased tidal volume and vital capacity. What is the most appropriate diagnosis?
Correct Answer : D
Motor neuron disease.
The involvement of respiratory muscles in MND is associated with poor respiration causing sleep apnoea.
Q.210. A young adult presents to the emergency department after a motorcycle crash. The patient has bruises around the left orbital area. GCS 13, examination notes alcoholic breath. Shortly afterwards, his GCS drops to 7. What is the most important initial assessment test?
Correct Answer : B
The likely cause is epidural haematoma
Q.211. A 32-year-old woman presents to the emergency department with headache and vomiting. She was decorating her ceiling that morning when the headache began, felt mainly occipital with neck pain. Some 2 hours later she felt nauseated, vomited and was unable to walk. She also noticed that her voice had altered. She takes no regular medications and has no significant past medical history. Exam: acuity, field and fundi are normal. She has upbeat nystagmus in all directions of gaze with normal facial muscles and tongue movements. Her uvulas deviated to the right and her speech is slurred. Limb exam: left arm past-pointing and dysdiadochokinesis with reduced pin prick sensation in her right arm and leg. Although power is normal, she can’t walk as she feels too unsteady. Where is the most likely site of lesion?
Correct Answer : D
Diagnosis is Lateral Medullary Syndrome.
There is a loss of pain and temperature sensation on the contralateral (opposite) side of the body and the ipsilateral (same) side of the face. There are associated cerebellar symptoms and other cranial nerve involvement.
Q.212. A 6-month-old baby had loss of consciousness after which he had jerky movement of hands and feet. What is the most probable diagnosis?
Correct Answer : D
In partial simple seizer there is no LOC (loss of consciousness). Infantile spasm though may be associated with occasional LOC but its nature is more generalized rather than the focal nature described here.
So the likely option is E. Partial complex seizure.
Q.213. A child has just recovered from meningitis. What investigation will you do before discharge?
Correct Answer : D
Deafness is a common complication of meningitis, so hearing the test is suggested before discharge.
Q.214. A 68-year-old woman has a sudden onset of pain and loss of hearing in her left ear and unsteadiness when walking. There are small lesions visible on her palate and left external auditory meatus. What is the most likely diagnosis?
Correct Answer : D
Herpes zoster infection
Q.215. For a patient presenting with Parkinson’s disease which of the following drugs is most useful in the management of the tremor?
Correct Answer : C
Benzhexol is the drug of choice in Parkinson’s disease-induced tremor.
Q.216. A man was brought to the emergency department from a shopping mall after collapsing there. He is conscious and answering questions now. His ECG shows irregular rhythm. Your choice of investigation?
Correct Answer : D
Echo may show clot in atrial appendage responsible for this attack of TIA secondary to atrial fibrillation.
Q.217. A 50-year-old man presents to the emergency department with acute back pain radiating down to his legs. Pain which is usually relieved by lying down and exacerbated by long walks and prolong sitting. What investigation would be the best option?
Correct Answer : A
Back pain radiating to the leg, pain relieved by lying down and exacerbated by long walks and prolonged sitting are characteristic of lumbar disc disease.
Q.218. A woman presented with blurred vision and intermittent clumsiness for 3 months. Reflexes are brisk in her arm and optic disc is pale. What is the most appropriate test to confirm diagnosis?
Correct Answer : C
Features are suggestive of multiple sclerosis. Investigation of choice is gadolinium enhanced MRI.
Q.219. A 63-year-old man presents after having a seizure. Examination: alert, orientated, in attention on the left side and hyperreflexia of the arm. What is the most probable diagnosis?
Correct Answer : A
Cerebral tumor
Q.220. A 50-year-old lady with weak limbs when examined was found to have burn marks on finger tips, wasted and weak hands with diminished reflexes. She also has weak spastic legs and dissociated sensory loss. What is the diagnosis?
Correct Answer : B
Syringomyelia.
Weak limbs, burn mark on fingertip (as pain and temperature sensation is lost due to spinothalamic tract damage), wasted and weak hands with diminished reflexes, weak spastic legs with dissociated sensory loss are features suggestive of Syringomyelia.
Common features are given below:
Sensory features:
1) loss of pain and temperature sensation
2) sensory loss is experienced over the arms, shoulders, and upper body
3) light touch, vibration, and position senses in the feet are affected as the syrinx enlarges into the dorsal column.
Motor features:
1) muscle wasting and weakness begin in the hands and then affect the forearms and shoulders.
2) tendon reflexes are lost. Autonomic involvement like bladder and bowel can occur.
Q.221. A-73-year old male presents with a 12 months history of falls. His relatives have also noticed rather strange behavior of late and more recently he has had episodes of enuresis. Examination: disorientation to time and place, broad-based, clumsy gait. What is the most probable diagnosis?
Correct Answer : D
Normal pressure hydrocephalus is a clinical symptom complex caused by the build-up of cerebrospinal fluid.
This condition is characterized by abnormal gait, urinary incontinence, and dementia. History of falls and broad-based clumsy gait (balance and gait disturbance), strange behavior, and episodes of enuresis (urinary incontinence) points towards normal pressure hydrocephalus.
The classic triad of normal pressure hydrocephalus: i) gait abnormality ii) urinary incontinence and iii) dementia.
Q.222. A 75-year-old nursing home resident complains of headache, confusion and impaired vision for 4 days. She has multiple bruises on her head. What is the most likely cause of confusion in this patient?
Correct Answer : C
Subdural hematoma.
Elderly patient with multiple bruises on her head suggests head injury which can lead to subdural hematoma.
Q.223. A 69-year-old woman has had a stroke. Her left upper and lower limbs are paralyzed and she is having difficulty in speaking. Which anatomical site is most likely affected?
Correct Answer : C
Hippocampal lesion causes mainly memory impairment.
The cerebellum has diagnostic features that are not present here. Thalamic lesions can lead to impairment of arousal, orientation, learning and memory, facial paresis, language deficit, hemispatial neglect, hemisensory loss, hemiparesis, hemiataxia, and visual field defect.
Brainstem stroke causes impaired consciousness, disorder of blood pressure, and breathing abnormality. The given picture is typical of the lesion in the internal capsule.
Q.224. A patient presents with gradual onset of headache, neck stiffness, photophobia and fluctuating LOC (loss of consciousness). CSF shows lymphocytosis but no organism on gram stain. CT brain is normal. What is the most likely diagnosis?
Correct Answer : B
Fungal meningitis can also present like this but it is much more rare. Moreover, negative gram stain excludes fungal causes here. Hence TB meningitis is the answer.
Q.225. A 74-year-old female presents with headache and neck stiffness to the emergency department. Following a LP the patient was started on IV ceftriaxone. CSF culture revealed listeria monocytogenes. What is the appropriate treatment?
Correct Answer : B
Change to IV amoxicillin + gentamycin.
From the given option B is the most acceptable. However, Ampicillin + gentamycin is the drug combination of choice.
Q.226. A 30-year-old man is suffering from fever, rash and photophobia. Doctors are suspecting he is suffering from meningitis. Which is the best medication for this condition?
Correct Answer : B
The patient is getting probable meningococcal meningitis. Before confirming the diagnosis suggested treatment is, where the organism is unknown:
So in a given case Cefotaxime is the option.
Q.227. A 42-year-old man has been tired and sleepy for the last few weeks in the morning. His work has started getting affected as he feels sleepy in the meetings. His BMI is 36. What is the most likely diagnosis?
Correct Answer : D
Day time somnolence and obesity (high BMI of 36) point the diagnosis of OSAS.
Q.228. A 35-year-old pregnant woman has been having tingling and numbness of her thumb, index and middle fingers for a while. She has been treated with local steroids but it hasn’t helped her much and now she has planned to undergo a surgical procedure. Which of the following structures will be incised?
Correct Answer : B
This is a case of carpal tunnel syndrome. So transverse carpal ligament is the structure that will be incised.
Q.229. Which of the following reflexes and innervating spinal nerves are correctly paired?
Correct Answer : D
Knee jerk – L3 & L4.
Anal reflex – S2-4;
Ankle jerk – S1-2;
Biceps jerk – C5-6;
Knee jerk – L3-4;
Triceps jerk – C7.
Q.230. A 68-year-old lady complains of falls to the ground without any warning, maintains consciousness and no confusion. She says this has occurred at number of times. What is the diagnosis?
Correct Answer : D
Drop attacks are sudden spontaneous falls while standing or walking, with complete recovery in seconds or minutes. There is usually no recognized loss of consciousness, and the event is remembered.
Q.231. A man sat cross-legged for about 30 minutes. After this he was unable to dorsiflex his left foot and had loss of sensation in the web space between the big toe and the 2nd toe. He also has sensory loss on the same side of the foot after 2 hour. Which of the following was affected?
Correct Answer : C
Common peroneal nerve winds around the fibular neck at knee joint and when a man sits cross-legged for a considerable time pressure is exerted on the the nerve may cause nerve palsy.
Q.232. An employer sent his worker to the emergency department after having hit his head on a machine. Examination: normal. What is the most likely investigation you would do?
Correct Answer : D
Indications for CT are not fulfilled by the given criteria for CT. As no sign of basal or skull fracture no need to do a skull X-ray.
Hence answer to this question is D. Reassurance.
Q.233. An 82-year-old woman has developed painful rash on one side of her forehead and anterior scalp. Lesions have also affected her cornea. What is the most appropriate option?
Correct Answer : D
Trigeminal nerve. Probable herpes zoster opthalmicus.
Q.234. A 66-year-old woman has been brought to the hospital on a number of occasions with a history of loss of memory. Her past medical history is significant for an MI 6yrs ago. It is noted that she has a step wise decline of her cognitive functions. What is the most likely diagnosis?
Correct Answer : B
Vascular dementia.
History of MI and stepwise decline of the cognitive function indicates vasculopathy and hence vascular dementia.
Q.235. A 62-year-old man who has recently had flu-like illness has woken to find his speech altered. Movement of his eyelids and lips are weak on the right side. Examination: normal. Which anatomical site is most likely to be affected?
Correct Answer : A
Facial nerve.
Viral infection is a common cause of facial nerve palsy.
Q.236. A 58-year-old man has a headache and confusion of 3 days after slipping and hitting his head in the garden. What is the most appropriate initial investigation?
Correct Answer : C
The likely diagnosis is subdural haematoma for which appropriate initial investigation is a CT scan of the brain.
Q.237. A woman previously in good health presents with sudden onset of severe occipital headache and vomiting. Her only physical sign on exam is a stiff neck. Choose the most likely diagnosis.
Correct Answer : A
Sudden onset severe occipital headache and vomiting with stiffness makes the likely diagnosis to be subarachnoid hemorrhage.
Q.238. A 34-year-old housemaid presents with headaches in the back of her head for several days and pain on flexing her neck. What is the most likely cause?
Correct Answer : B
Headache in the back of head and pain in flexing neck is an early feature of cervical spondylosis which gradually progresses to later symptoms like radiculopathies due to root compression in arms and hands.
Q.239. A 75-year-old man on digoxin develops weakness in the right upper and lower limbs which resolves within a few hours. What is the most definitive investigation for this condition?
Correct Answer : C
Patient on digoxin means he is being treated for atrial fibrillation with heart failure and the cause of TIA is cardiac in origin!
So carotid Doppler or carotid angiography is not the answer. Again for TIA investigation of choice is MRI if not CT. So for this question definitive investigation is CT scan.
Q.240. A 35-year-old man presents with balance problems, headache, SNHL (sensory neural hearing loss) and loss of corneal reflex on the left side. What is the most definitive investigation?
Correct Answer : C
Probable diagnosis is left sided acoustic neuroma. For this most definitive investigation is MRI internal auditory meatus.
Q.241. A 42-year-old female had sudden severe headache and vomiting. She took paracetamol and then collapsed. What is the most likely diagnosis?
Correct Answer : A
Sudden headache, vomiting, collapse are suggestive of SAH.
Q.242. A 60-year-old man was brought in by his wife complaining of ataxia, urinary incontinence and erectile dysfunction. He also complains of rigidity and slowing of movement with a pill rolling tremor of the hands. What is the likely diagnosis?
Correct Answer : C
Shy-drager syndrome is characterized by parkinsonism (rigidity, slowing of movement with hand tremors) plus a more pronounced failure of the autonomic nervous system (urinary incontinence and erectile dysfunction) and there may also, cerebellar signs like ataxia are present.
Q.243. A 17-year-old has acute pain around his right eye, pain on one side of his face and ear ache too. What is the most likely diagnosis?
Correct Answer : D
It seems to be herpes zoster of the trigeminal nerve. Onset is acute, unilateral distribution favours herpes zoster.
Most likey early stage of Ramsay hunt syndrome.
Q.244. A 31-year-old man underwent an operation where his hand was hanging outside the table. After the operation he had wrist drop and sensory loss over the dorsum of his hand. Which nerve was injured?
Correct Answer : A
As the man’s hand was hanging outside the ot table there was pressure on the radial nerve at arm level which is similar lesion of Saturday night palsy.
Q.245. A 64-year-old man presents with ipsilateral vertigo, tinnitus and left sided hearing loss. Examination: Rinne test +ve and Weber’s lateralizes to the right ear. What is the most appropriate investigation?
Correct Answer : B
Rinne positive, so it is not conductive deafness. Again we know if Weber lateralizes to a deaf ear it is conductive and lateralized away from a deaf ear then it is sensory neural. So here there is sensory neural hearing loss in the left ear. So the most appropriate investigation is MRI brain.
Q.246. A 23-year-old man sprained his right ankle 6 weeks ago while playing football. He was treated with a below knee walking cast. On removal of the cast, the patient noted to have right foot drop. He has weakness of extensors of the ankle and toes and diminished pin prick sensation over the dorsum of the foot. The ankle jerk is present and plantar reflex is flexor. What is the most likely cause of the foot drop?
Correct Answer : A
Foot drop, weakness of extensors of the ankle and toes and diminished pin prick sensation over the dorsum is suggestive of compression of common peroneal nerve.
Q.247. A 3-year-old girl presents with complains of sudden right facial weakness and numbness and pain around her ear. There are no symptoms. What is the most appropriate diagnosis?
Correct Answer : B
Bell’s palsy.
Q.248. A 33-year-old female complains of diplopia on upright gaze. Examination : Ptosis can be seen. There are no other complains or any significant PMH (past medical history). What is the most appropriate investigation for him?
Correct Answer : D
A case of 3rd nerve palsy. So to delineate the cause CT should be done.
Q.249. A 68-year-old patient wakes up with slurred speech and right sided weakness. CT shows cerebral infarct. What is the most appropriate treatment?
Correct Answer : A
The window period to administer alteplase is 4.5 hours. If we cannot certain (here patient was sleep, so period is not possible to establish) this period we cannot proceed for alteplase.
Q.250. A 73-year-old man who is recovering from surgery on the left carotid artery in his neck. He has slurred speech. On protrusion of his tongue, the tip deviated to the left. What is the most appropriate option?
Correct Answer : D
Testing function of the nerve is performed by asking the subject to stick their tongue straight out. If there is a loss of innervation to one side, the tongue will curve toward the affected side, due to unopposed action of the opposite genioglossus muscle.
If this is the result of a lower motor neuron lesion, the tongue will be curved towards the damaged side, combined with the presence of fasciculations or atrophy. However, if the deficit is caused by an upper motor neuron lesion, the tongue will be curved away from the side of the cortical damage, without the presence of fasciculations or atrophy.
Q.251. A 45-year-old male complains of tremors in hands. Examination: tremors are absent at rest but present when arms are held outstretched and persist on movement. What is the most probable diagnosis?
Correct Answer : B
Tremors absent at rest and present on outstretched hand and persist on movement are benign essential tremors.
Q.252. A 24-year-old male involved in RTA with X-ray showing fracture neck of humerus. What is the associated nerve injury?
Correct Answer : A
Axillary nerve
Q.253. An 82-year-old man has woken up with incoherent speech and difficulty in finding the right words. Examination: otherwise normal, good comprehension. Which anatomical site is most likely to be affected?
Correct Answer : A
A person with expressive aphasia will exhibit halting and effortful speech. Speech may only include important content words. Word comprehension is preserved. The person may still be understood, but sentences will not be grammatical.
This contrasts with receptive or Wernicke’s aphasia, which is distinguished by a patient's inability to comprehend language or speak with appropriately meaningful words though fluency may be preserved.
Q.254. A-34-year old male presents with headache and vomiting. Examination: temperature 38.5C, neck stiffness, discharge from left ear and right sided hyper-reflexia with an extensor plantar response. What is the most likely diagnosis?
Correct Answer : D
Otitis media can lead to cerebral abscess.
Q.255. A 26-year-old male presents with speech difficulties. Examinations: nystagmus. Which anatomical site is most likely to be affected?
Correct Answer : C
Difficulty speech (cerebellar dysarthria) and nystagmus are suggestive of cerebellar lesion.
Q.256. A 50-year-old man complains of visual problems and dull pain in the left eye. Fundoscopy reveals papilloedema. He was diagnosed with MS 2yrs ago. There is no consensual light reflex of the right eye. What is the single most likely defect?
Correct Answer : B
Mono-ocular field loss
Q.257. A 54-year-old patient wakes up with right sided weakness. His current medication is bendroflumethiazide for HTN (hypertension). Pulse 92 bpm, BP 160/90mmHg. CT shows left cerebral infarct. What is the most appropriate treatment?
Correct Answer : B
In stroke window period to use alteplase is 4.5 hours. In the given history we can in no way be certain the time of stroke and we can not proceed for alteplase unless the window period is confirmed. Hence we cannot give alteplase but Aspirin.
Q.258. A 33-year-old man presented to the GP with history of headaches and photophobia. The GP examines him and finds a rash. What's the best next step in management?
Correct Answer : B
Before hospitalization IV benzylpenicillin. In hospital Ceftriaxone can be given but not in calcium-containing fluid instead Cefotaxime.
Q.259. A 42-year-old man presents with stroke. He is not able to walk straight and his speech is slurred. What is the initial appropriate investigation?
Correct Answer : A
Ataxia and slurred speech are features of cerebellar lesion which is the posterior fossa organ. For posterior fossa lesions MRI is the investigation of choice.
Q.260. A 35-year-old woman presents with visual problems. CT brain reveals pituitary tumor. What is the most likely defect?
Correct Answer : C
Bitemporal hemianopia. Pituitary tumour by pressing optic chiasma causes bitemporal hemianopia.
Q.261. A young lady presents with gradually worsening headaches, visual disturbance, and lack of energy. MRI shows 15mm tumor in the pituitary fossa. What is the treatment of choice?
Correct Answer : D
Hormonically active tumour, tumour causing pressure symptoms (like headache, visual disturbance) and large size of tumour are indications for surgical removal.
Q.262. A 50-year-old man with a known history of stroke. He can’t remember anything about his life. What is the most likely defect?
Correct Answer : B
Memory processing occurs in the temporal lobe. So as the patient lost memory his temporal lobe is involved. We know temporal lobe lesion causes “homonymous upper quadrantanopia” which is the key here.
Q.263. A 75-year-old woman has weakness of the left side of her face. She has had a painful ear for 48 hours. There are pustules in the left ear canal and on the eardrum. What is the most likely diagnosis?
Correct Answer : B
A case of Ramsay Hunt syndrome defined as an acute peripheral facial neuropathy associated with erythematous vesicular rash of the skin of the ear canal, auricle (also termed herpes zoster oticus), and/or mucous membrane of the oropharynx caused by Herpes zoster infection.
Q.264. A 45-year-old lady presents with history of double vision and facial numbness. Which anatomical site is most likely to be affected?
Correct Answer : D
Cerebral cortex will not cause features of cranial nerve lesions.
Trigeminal nerve: ophthalmic and maxillary divisions are pure sensory hence it is also not the answer. Oculomotor does not cause facial numbness. These features are not of basal ganglia lesions also. These features only can be explained by cranial nerve involvement in brainstem lesion.
Q.265. A 65-year-old lady presents with a 6 hours history of facial droop and weakness in the left side of her body. What single agent will she be prescribed for her whole life?
Correct Answer : A
For both TIA and stroke Clopidogrel is prescribed for life long if there are no drug allergies.
Q.266. A man with history of fall had confusion and laceration mark on the head. Which is the vessel affected?
Correct Answer : B
Considerable head injury and lucid interval (several episodes of transient confusion) points towards extradural hematoma which occurs frequently from bleeding from the middle meningeal artery. A subdural hematoma usually occurs due to bleeding veins.
Q.267. A 56-year-old patient has been diagnosed with MS (multiple sclerosis). She presents with a positive Romberg’s test. She also has weakness and loss of sensations in all her 4 limbs. Which site is most likely to be affected?
Correct Answer : C
Cervical spinal cord.
Quadriplegia is the feature of cervical cord lesion.
Q.268. A 32-year-old woman suffers an episode of severe occipital headache with vomiting and LOC (loss of consciousness). She is brought to the hospital where she is found to be conscious and completely alert. Examination: normal pulse and BP with no abnormal neurological sign. What is the next step in her management?
Correct Answer : B
To exclude any possible intracranial bleeding.
Q.269. A 74-year-old man presents with sudden onset of with right sided weakness and slurred speech. He also has loss of sensation over the right side of the body and visual field defects. CT shows ischemic stroke. What is the most appropriate management?
Correct Answer : A
If no time frame is mentioned it is assumed that the patient arrived at window period unless given evidence of uncertain time like a stroke after getting up from sleep. Aspirin is started at least after 24 hours of giving alteplase.
Q.270. A 67-year-old man presents with a history of increasing confusion and drowsiness. He had a fall 2 weeks ago. CT head reveals a chronic subdural hematoma. What is the best management for this patient?
Correct Answer : B
Burr hole drainage.
Q.271. A 49-year-old man first presented with increasing difficulty in swallowing. Several months later he developed weakness in his right foot. Now he can no longer feed himself, he chokes on food and has become confined to a wheelchair. What is the most likely diagnosis?
Correct Answer : D
The picture is of amyotrophic lateral sclerosis with bulbar onset, so it has a very bad prognosis.
Q.272. A patient with vesicles in the maxillary division of trigeminal nerve. Which area of mucus membrane will be involved?
Correct Answer : B
Cheek.
Q.273. A 52-year-old man presents with visual hallucinations and features of cognitive impairment. What is the most likely diagnosis?
Correct Answer : B
Visual hallucinations and cognitive impairment are suggestive of Lewy body dementia.
Hallucination is a more prominent feature of LBD than Alzheimer's. Again cognitive impairment goes more with LBD while prominent early memory loss symptom suggests Alzheimer’s.
Q.274. A 24-year-old woman presents with tingling and twitching of her fingers followed by throbbing unilateral headache. What is the most likely diagnosis?
Correct Answer : B
The tingling and twitching of her fingers are aura and the migraine is with aura.
Q.275. A man suffers from Herpes Zoster affecting his face. Which of the following mucus membrane is to be affected?
Correct Answer : C
Conjunctiva
Q.276. A 24-year-old man after a head injury presents with difficulty dressing himself, difficulty in writing and inability to differentiate the fingers of his hand. Which part of the brain is most likely to be affected?
Correct Answer : A
Dressing apraxia, agraphia and finger agnosia are features of parietal lobe lesions.
Q.277. A patient had a stroke. Now, there is left sided weakness and right sided facial numbness. CT shows ischemic stroke. Which one would you prescribe?
Correct Answer : A
Alteplase
Q.278. A 73-year-old stroke patient has been on aspirin for 2 years. He now presents with epigastric pain and is asking for a treatment. What is the most appropriate management?
Correct Answer : C
Omeprazole
Q.279. A 32-year-old male complains of tremors everytime he tends to use his muscles and when he is pointing at objects. No complaints at rest. His father complained of similar problems. What is the most probable diagnosis?
Correct Answer : D
In benign essential tremor there is no rest tremor but tremor occurs during movement of the affected limb.
Q.280. A 40-year-old woman with breast cancer has back pain which keeps her awake at night. She blames it on a gym session she had 2 weeks ago. She now has difficulty in climbing stairs. There is tenderness over the right thoracic spine. She has diminished fine touch and temp sensation in her right foot. What is the most appropriate investigation?
Correct Answer : C
There is a neurological deficit, so to exclude spinal involvement MRI is the single most appropriate investigation.
Q.281. A 68-year-old man awoke to find that he is unable to close his left eye and dribbling saliva from the left angle of his mouth. What is the most appropriate option?
Correct Answer : A
Features are suggestive of left sided facial nerve palsy.
Q.282. A-63-year old male presents after having had a seizure. Examination: alert and oriented, inattention on the left side and hyperreflexia of the arm. What is the most probable diagnosis?
Correct Answer : A
Cerebral tumour
Q.283. A 67-year-old female presents with balance problems. Examination: nystagmus on left lateral gaze, a loss of the left corneal reflex and reduced hearing in the left ear. What is the most likely diagnosis?
Correct Answer : B
Acoustic neuroma.
Nystagmus, loss of corneal reflex, hearing loss, balance the problem is a well-known feature of acoustic neuroma.
Q.284. A 72-year-old male presents with acute confusion. He has been in the hospital for 2 weeks having been treated for a DVT. The nurses have noticed that he became increasingly drowsy. Examination: small scalp laceration, a GCS of 8 and bilateral upgoing plantar response. What is the likely diagnosis?
Correct Answer : D
Subdural hematoma.
Even trivial head trauma can lead to subdural hematoma. Presence of small scalp laceration, confusion, and becoming increasingly drowsy.
Glasgow coma scale of 8 is suggestive of subdural hematoma.
Q.285. A 69-year-old woman presents with a sudden onset of weakness of her right arm and leg. She is known to be hypertensive. There has been no headache, LOC (loss of consciousness), visual, speech or sensory symptoms. Examination: BP 180/90mmHg, pulse 100 and regular heart sounds, no carotid bruit. Higher mental function tests are normal. No apraxia or neglect. Speech, swallowing and sensation are normal. There are no visual field defects. There is a mild facial weakness sparing the forehead. The right arm and leg are flaccid and weak. Reflexes and tone are normal. There is a right extensor plantar response. What is the most likely cause of this pt’s symptoms?
Correct Answer : B
Weakness of right arm and leg. So lesion is on the left side.
Hence C, D can not be the option.
Also, no AF or carotid artery disease, and features are very much consistent with lacunar infarct.
Q.286. A 74-year-old man has been admitted unconscious with no history. He has a GCS (Glasgow coma scale) of 6 and a dilated left puil which becomes insensitive to light. What is the most likely diagnosis?
Correct Answer : D
Extradural hematoma is very rare in the elderly and there occurs lucid interval;
Features are not consistent with meningitis. Opioid and pontine hemorrhage causes myosis. So likely diagnosis here is SAH.
Q.287. A 27-year-old man presents to the emergency department with 2 days history of severe headache and pyrexia (38.9C). CT: petechial hemorrhage in the temporal and inferior frontal lobes. What is the most likely diagnosis?
Correct Answer : D
Petechial hemorrhage in the temporal and inferior frontal lobes are characteristic of Herpes simplex encephalitis.
Q.288. A 44-year-old woman with memory loss, poor concentration and inability to recognize household projects. She has right-handed involuntary writhing movement. There is strong family history of similar complain. What is the most likely diagnosis?
Correct Answer : C
A person with Huntington's disease may appear to have a lack of drive, initiative, and concentration. Involuntary jerking or writhing movements (chorea). Typical presentation is between 35-55 yrs.
Q.289. A 54-year-old man has collapsed suddenly following a headache. He has hypertension and takes warfarin for prosthetic heart valve. GCS 4 and dilated left pupil. What is the most likely diagnosis?
Correct Answer : C
Intracerebral hemorrhage.
Headache, collapse, and warfarin use make the diagnosis of intracerebral hemorrhage most likely.
Q.290. A 71-year-old man with no previous history is brought to the emergency department by his wife who says he has become progressively more forgetful, tends to lose his temper and is emotionally labile. There is no history of infectious disease or trauma. What’s the most likely diagnosis?
Correct Answer : D
Alzheimer’s disease.
Pic’s dementia and frontotemporal dementia are similar in some way (first personality change then dementia) but in Pic’s there is odd social behavior like violating etiquette and saying something vulgar.
In Huntington’s disease, there are changes in personality, cognition, and physical skills at the age of 35-45yrs and there is chorea.
In vascular dementia, there are multiple progressive infarcts and so neurological features may be associated with features of other vascular disease.
Q.291. An 82-year-old woman has been admitted from a nursing home with dense hemiplegia and homonymous hemianopia. She is dysphasic. What vessel is most likely to be involved?
Correct Answer : B
Mid cerebral artery.
Hemiplegia, homonymous hemianopia, and dysphasia are common features of mid-cerebral artery stroke.
Q.292. A man brings his wife into the emergency department after finding her unconscious at home. He says at breakfast time she had complained of sudden severe headache. What is the most appropriate investigation?
Correct Answer : C
Probable SAH. Among the given option most appropriate is CT brain.
Q.293. A 34-year-old female presented with vomiting preceded by an occipital headache of acute onset. Examination: conscious and alert with photophobia but no neck stiffness. CT: normal. What is the most appropriate further management?
Correct Answer : C
Probable subarachnoid hemorrhage.
CT may not show any abnormality in the early stage in some instances and in that case we shall do CSF examination 12 hours later to see xanthochromia.
Q.294. A 19-year-old man with known history of OM (otitis media) presents with headache, lethargy, sweating and shivering. What is the most likely diagnosis?
Correct Answer : B
Meningitis. OM often can be a cause of intracranial extension leading to cerebral abscess or meningitis.
Q.295. A 76-year-old woman presents with deep stroke 6 hours ago. What would the immediate treatment be?
Correct Answer : B
Aspirin 300mg
Q.296. A 50-year-old man with a known history of stroke is unable to get out of his house because he can’t find where the door is. He refuses help from his wife and says he is not blind. What is the most likely defect?
Correct Answer : D
Cortical blindness is the total or partial loss of vision in a normal-appearing eye caused by damage to the brain's occipital cortex. Rarely, a patient with acquired cortical blindness may have little or no insight that they have lost vision, a phenomenon known as Anton–Babinski syndrome.
Q.297. A camel rider sustained a kick to the lateral side of his right leg just below the knee caused by the camel stick. The site is slightly bruised and tender to touch. During physical examination, he is unable to either dorsiflex or evert the foot. There is loss of sensation over the front and outer half of the leg and dorsum of the foot. If these observations are the result of damage to a nerve bundle, which is the most likely nerve affected?
Correct Answer : B
Inability of dorsiflex and foot eversion with sensory loss over front and outer half of leg and dorsum of foot are seen in peroneal nerve injury.
Q.298. A 78-year-old man has collapsed. He has had a severe headache for 12 hours and had an URTI (upper respiratory tract infection) 3 days ago. He has a temperature 39.2C, pulse 122 bpm, BP 84/60 mmHg and RR 34 bpm but his chest is clear. He has a GCS 10 and some neck stiffness. He has been started on high-flow oxygen. What is the most appropriate immediate management?
Correct Answer : D
Patient is in shock and has probable meningoencephalitis. So at this point most appropriate immediate management is IV fluid and IV antibiotics.
Q.299. A 32-year-old woman has had 3 episodes of slurred speech and 2 episodes of transient weakness of both legs in the past 5 years. Each episode has resolved in 3 months. What is the most likely diagnosis?
Correct Answer : C
Multiple sclerosis
Q.300. A 55-year-old chronic alcoholic with known hepatic cirrhosis has been on a heavy bout of alcohol the night before and was brought home by friends after falling several times in the pub. While being taken up the stairs to his bedroom he falls down the flight of 5 steps but sustains no obvious injuiry. His wife calls the emergency department the next day because she could not rouse him in the morning. He is brought in in a comatose state and both pupils appear dilated. Skull vault XR appears normal. What's the diagnosis?
Correct Answer : B
Acute subdural hematoma, typical history of alcoholics, falls and usually debilitated or elderly, hepatic cirrhosis increases coagulopathy and chances for bleed.
Q.301. A young man develops nonfluent, effortful speech with dysarthria. He is able to understand speech. He fails to repeat the sentence. What would you do next?
Correct Answer : D
MRI's Frontal lobe (Brocas area).
Production (Broca's) dysphasia / aphasia - lesions are located in the left pre-central areas.
Q.302. Titubation is a feature of disease involving?
Correct Answer : A
Titubations (head/body nodding) mostly occur due to cerebellar lesions.
Q.303. A 30-year-old caucasian man presented with a 2 weeks history of gradually worsening vision in his left eye. The patient had been seen once by a neurologist 2 years previously for flashes. At that time a head CT was normal. The patient was lost to follow up with the neurologist, but the flashes had continued for the 2 year period. The patient did not experience visual changes with activity or movement. The patient reported continued decreasing vision. Goldmann visual fields were done and showed a central scotoma. An MRI was done at this time and showed inflammation of the left optic nerve. The likely diagnosis is?
Correct Answer : C
Possible diagnosis is MS (multiple sclerosis). Scotoma, 2 year history, age race are suggestive except more in females than males.
Q.304. A 23-year-old male presents to his GP 2 weeks after a RTA (road traffic accident) concerned about increasing anxiety lethargy and headache. At the time he had a CT brain after banging his head on the steering wheel, which revealed no abnormality. 6 months following this episode his symptoms have resolved. What did his original symptoms likely represent?
Correct Answer : D
Post-concussion syndrome is a set of symptoms that may continue for weeks, months, or a year or more after a concussion – a minor form of traumatic brain injury.
Q.305. A 62 year old woman has right-sided headaches with malaise, weight loss and depression. What is the most appropriate investigation?
Correct Answer : A
Right-sided (one-sided) headache with malaise, weight loss, and depression in 62 yrs elderly is highly suggestive of temporal arteritis for which “SINGLE” most appropriate investigation is temporal artery biopsy. If asked most appropriate answer would be ESR.
Q.306. A 56-year-old man has sudden severe occipital headaches, drowsiness and vomiting. What is the most initial appropriate investigation?
Correct Answer : A
Sudden severe occipital headaches, drowsiness, and vomiting are highly suggestive of SAH. Here single most appropriate investigation is a CT scan of the brain.
Q.307. A 45-year-old woman has right sided headaches, nausea and visual disturbance. This lasted for 24 hours and she is fine. She was recently started on hormone replacement therapy. What is the most initial appropriate investigation?
Correct Answer : C
One-sided headache lasting for 24 hours associated with nausea and visual disturbance without any focal neurological sign is highly suggestive of migraine. So for this “no investigation is needed”.
Q.308. A 20-year-old woman with multiple sclerosis presents with blurring of vision and pain in the eye on movement. Where is the lesion?
Correct Answer : C
Optic neuritis is a well-known feature of multiple sclerosis. The described lesion is optic neuritis!
Optic neuritis is a demyelinating inflammation of the optic nerve. It is also known as optic papillitis (when the head of the optic nerve is involved) and retrobulbar neuritis (when the posterior of the nerve is involved).
Q.309. A 65-year-old man after an open cholecystectomy experiences numbness around the umbilicus. Which nerve is damaged?
Correct Answer : D
Dermatome pattern of T10 nerve: Traverses posteriorly from T10 to anteriorly through the umbilicus.
Q.310. A 23-year-old lady with multiple sclerosis presents with ataxia, dysarthria and nystagmus. Which of the following is the most likely location of the lesion?
Correct Answer : C
Ataxia, dysarthria and nystagmus are well known features of cerebellar lesion.
Choose a Question
×Choose a Question
×
Trial Access Limit Reached
You’ve reached the limit of free content. Subscribe to continue learning without restrictions.